


L4-L5 Slip Disc Care Without Surgery in KL & PJ
L4-L5 slip disc care in Kuala Lumpur, KL, and Petaling Jaya focuses on a part of the lower back that handles frequent sitting, bending, lifting, and daily load transfer. The L4-L5 disc sits close to the pelvis and nearby nerve pathways, so spinal joint or disc damage (slip discs) here may affect the lower back, buttock, thigh, or leg. Common L4-L5 findings include disc bulge, herniation, and early wear. Some people notice stiffness in the lower back, while others notice tingling, pulling, or changes in how they stand and walk.
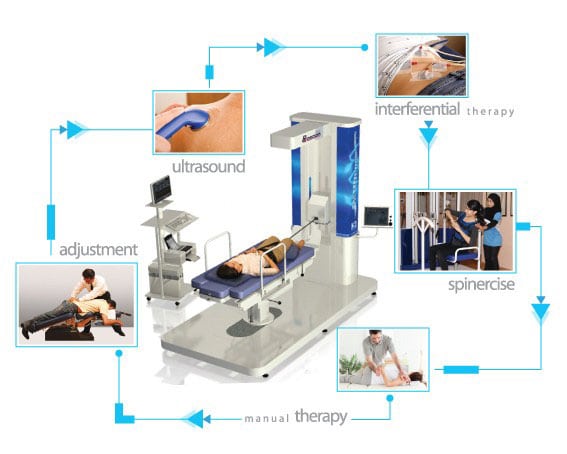
In KL and PJ, care often begins with a detailed look at posture, spinal control, and how the body handles daily activity. At Chiropractic Specialty Center®, gentle and focused methods may include chiropractic joint mobilization, physical therapy, and guided rehabilitation based on individual findings.
7 Key Takeaways of L4-L5 Spinal Issues
- L4-L5 slip disc damage are common and may include disc bulge, protrusions, prolapsed, or herniation, early wear, facet hypertrophy, ligamentum flavum thickening, and sometimes spondylolisthesis.
- Symptoms are not always limited to the lower back. L4-L5 spinal disc issues or joint disorders may affect the buttock, thigh, calf, foot, walking tolerance, balance, or leg control.
- Assessment matters before hands-on care. MRI findings, nerve-related symptoms, posture, walking pattern, and daily load tolerance all help guide what needs more caution.
- Forceful twisting, repeated cracking, or unassessed manual care may not suit every L4-L5 presentation, especially when disc damage such as bulges and extrusions (slipped discs), nerve symptoms, facet overgrowth, or ligament thickening are already present.
- L4-L5 problems often involve more than one structure at the same time. Disc issues, facet joint enlargement, ligament thickening, and segmental instability may occur together and narrow the available space for nearby nerves.
- Not every invasive option is strongly supported by long-term evidence. Your page now explains why some patients benefit more from a careful conservative-first discussion before jumping to more aggressive procedures.
- For people in KL and PJ, the most useful starting point is a structured review of symptoms, imaging, movement, spinal control, and daily activity demands.
Video: Sciatica vs Slipped Disc — How to Tell the Difference
If symptoms travel from the lower back into the buttock, thigh, calf, or foot, the first question is not always whether the problem is the sciatic nerve alone. In many cases, the real source is higher up at the L4-L5 disc or nearby nerve roots. In this video, Yama Zafer explains how to tell the difference between L4-L5 sciatica, nerve irritation, and a slipped disc pattern, and why the spinal source matters before choosing care.
Key Moments for This Video on Sciatica and Spinal Disc Damage
- 00:00 Why sciatica is a symptom pattern, not a stand-alone diagnosis
- 01:15 How L4, L5, S1, and S2 roots form the sciatic nerve
- 02:30 Why many leg symptoms begin with a lumbar disc issue
- 05:45 Sitting, walking, posture, and daily load at the lower back
- 10:00 Why forceful cracking may need more caution in disc-related sciatica
- 11:00 When surgery may be discussed versus conservative-first care
L4-L5 Guide: 7 Signs, Sciatica, Stenosis, MRI, and Nerve Symptoms
Lumbar Disc Levels Explained: L1-L2 to L5-S1
Lower back issues do not affect every spinal level in the same way. An L1-L2 problem may behave very differently from an L4-L5 or L5-S1 issue because each segment handles load, movement, and nerve involvement differently. That is why this lumbar guide series looks at each level separately, from the upper lumbar spine down to the lumbosacral junction.
Use the pages below to understand how symptoms, slip disc (prolapses, protrusions and bulges), joint stress, and nerve-related findings may differ by level:
- L1–L2 Spinal Joint, Disc & Nerve Care in Kuala Lumpur: Upper lumbar problems and disorders such as facet joint disorders or spinal disc issues at L1-L2 may affect the low back, groin, hip region, and nearby nerve pathways in ways that differ from lower lumbar disc problems.
- L2-L3 Disc Bulge Care – A Non-Surgical Approach: L2-L3 disc issues (bulges, herniations & protrusions) may affect the front of the thigh, hip flexor function, and walking comfort, especially when nerve irritation is present.
- L3–L4 Spine Care in Kuala Lumpur: L3-L4 problems may influence the front of the thigh, knee region, leg strength, and day-to-day movement tolerance.
- L4-L5 Disc Care Without Surgery In KL & PJ: L4-L5 spinal segment is one of the busiest spinal levels and is often linked with slip disc findings, sciatica, stenosis, foot weakness, and walking-related leg symptoms.
- L5-S1 Disc Issues – Targeted Non-Invasive Care: L5-S1 commonly affects the buttock, calf, heel, and foot, and may play a major role in disc-related sciatica and lumbosacral load stress.
Together, these pages help explain how each lumbar level can affect the back, pelvis, leg, foot, and nearby nerve structures differently, and why careful level-specific assessment matters.
L4-L5 Disc Bulge Symptoms: How It Affects Your Back, Leg, and Movement
The L4-L5 disc sits just above the L5-S1 segment and close to the pelvis, making it one of the busiest parts of the lower back during sitting, bending, lifting, and walking. Because of its position and daily workload, changes at the L4-L5 disc may affect nearby back joints and nerves. This is why some people notice lower back stiffness, leg symptoms, or changes in how they stand, walk, and move during the day.
As the disc changes shape (degenerates, bugles and herniates) or loses support, the body may begin to compensate. Some people notice stiffness in the lower back, while others feel sensations traveling into the buttock, thigh, or lower leg. In some cases, balance, walking pattern, or leg control may feel different, especially after sitting or standing for longer periods.
Contact the Nearest Chiropractic Specialty Center in KL :
- In KL visit our Bukit Damansara: WhatsApp: +60 12 510 5600
- Our PJ and KL center in Bandar Sri Damansara: WhatsApp: +60 12 455 6939
Common L4-L5 Disc Symptoms to Watch For

- Lower back stiffness: Often felt after sitting, bending, or staying in one position for too long
- Sensations into the leg: Tingling, pulling, or heat-like feelings moving into the buttock, thigh, or lower leg
- Position-related changes: Symptoms may increase with sitting or walking and ease when lying down
- Changes in leg control: A feeling of heaviness or reduced control in the foot or ankle in more advanced cases
Sciatica: Why Slip Disc Can Affect the Buttock, Thigh, Calf, or Foot
L4-L5 sciatica usually happens when slip-disc-related issues at the L4-L5 level begin to affect nearby nerve structures. That may happen through disc bulge, herniation, narrowing around the nerve space, or a combination of disc degeneration, slippage, or disc ruptures with facet hypertrophy or ligament thickening. When that happens, symptoms may move beyond the lower back and into the buttock, thigh, calf, or foot.
Not every person with an L4-L5 bulged disc develops sciatica, and not every leg symptom means the same thing. Some people notice tingling or pulling into the thigh. Others notice calf symptoms, foot heaviness, or reduced walking tolerance. Symptoms may increase with sitting, bending, standing for longer periods, or walking, especially when the segment is already handling load poorly.

The reason this matter is that L4-L5 sciatic pain issues often points to more than simple stiffness. It may reflect irritation or crowding around the nerve pathway. That is why assessment matters more once leg symptoms begin to travel farther down, become easier to trigger, or start affecting balance, walking, or foot control.
Common Sciatica Patterns
- Symptoms moving from the lower back into the buttock or thigh
- Tingling, numbness, or pulling into the calf or foot
- Heaviness in the leg during walking or standing
- Symptoms that ease somewhat with rest or position change
- Reduced tolerance for sitting, driving, or longer walks
L4-L5 Nerve Compression: Why Tingling, Numbness, Weakness, or Sciatica May Develop
L4-L5 nerve compression happens when nearby nerve tissue becomes irritated, compressed, inflamed, or all three at the same time. This is different from simply saying the canal is narrow. spinal stenosis describes the crowded space. L4-L5 nerve compression describes what that crowding, disc change, or foraminal narrowing is actually doing to the nerve.
At the L4-L5 level, symptoms may develop through two main mechanisms. The first is mechanical pressure, where a disc bulge, herniation, facet overgrowth, or narrowing around the nerve space physically compresses or stretches the nerve. The second is biochemical irritation, where inflammatory disc material and surrounding cytokine activity make the nerve more sensitive and reactive. Recent clinical review literature supports this broader view and explains why symptom intensity does not always match the size of a disc bulge or the amount of visible narrowing on MRI.
This is why sciatica (sciatic nerve pain)may feel burning, electric, sharp, or traveling. It is also why tingling, numbness, and weakness can appear in different combinations. Tingling may reflect irritated or unstable nerve signaling. Numbness may reflect reduced sensory signal transmission. Weakness may happen when motor fibers are not conducting normally, especially when the compression or inflammatory irritation has started to affect muscle control more clearly. At L4-L5, this may influence the outer leg, top of the foot, big toe region, or the ability to lift the foot and toes during walking. The same paper also emphasizes that clinical findings and imaging need to be read together, not in isolation.
Common Signs That May Suggest L4-L5 Nerve Compression
- Tingling, burning, or electric-like sensations into the buttock, thigh, calf, or foot
- Numbness over the outer leg, top of the foot, or big toe region
- Sciatica that becomes easier to trigger with sitting, bending, standing, or walking
- Heaviness in the leg or reduced confidence during walking
- Weakness in foot lift, toe lift, or heel walking
Foot Drop: When Weakness Needs Faster Attention
foot drop is one of the more important motor changes to watch for because it may suggest that nerve involvement is starting to affect muscle control more clearly. At this level, weakness may affect foot dorsiflexion and great toe extension, which can make heel walking harder or make the foot feel slow, heavy, or difficult to lift during walking. In the JOR Spine review you shared, weakness in foot and first-toe dorsiflexion is highlighted as one of the more useful clinical indicators for this pattern of nerve root involvement.
When that kind of weakness appears, the question is no longer just whether the lower back is irritated. The more important issue is whether the nerve is being affected enough to change function. That is why L4-L5 foot drop, worsening weakness, or a clear change in walking pattern deserves faster medical assessment.
Reference for Nerve Compression and Foot Drop
- Sima S, Diwan A. Contemporary clinical perspectives on chronic low back pain: The biology, mechanics, etc. underpinning clinical and radiological evaluation. JOR Spine. 2025;8(1):e70021. Published 2025 Jan 23. doi:10.1002/jsp2.70021.
When L4-L5 Symptoms Can Be Monitored and When Assessment Matters
Some L4-L5 symptoms stay mild and come and go. Others begin to affect daily activity more clearly.
Symptoms That May Be Monitored
- Mild stiffness that improves with rest or position changes
- Occasional leg sensations that do not keep spreading
- No clear change in walking, balance, or foot control
When Assessment Is Recommended
- Symptoms lasting more than a few days without improvement
- Repeated episodes affecting sitting, standing, or walking
- Sensations traveling further into the calf or foot
- Tingling, numbness, or heaviness that is becoming easier to notice
When More Urgent Medical Evaluation Is Needed
- Sudden change in leg control
- Difficulty lifting the front of the foot
- Major change in walking balance
- Change in bowel or bladder function
Non-Surgical L4-L5 Slip Disc Care in Kuala Lumpur & Petaling Jaya
In Kuala Lumpur and Petaling Jaya, care for L4-L5 disc concerns often focuses on how the spine handles load during daily activity. A structured approach may include chiropractic joint mobilization, physical therapy, and guided rehabilitation.
At Chiropractic Specialty Center®, care begins with a detailed look at movement, posture, and spinal control. Gentle and focused methods are used to reduce stress on the disc while improving coordination between the spine, muscles, and joints over time.
Muscle and Ligament Disorders at L4-L5
Muscular and ligamentous issues at the L4-L5 level are commonly associated with damage, wear, or trauma. Ligamentum flavum, a ligament with muscle-like properties, can become damaged or hypertrophied (thickened), compressing nerves and contributing to lower back issues. While age-related degeneration of ligaments and muscles is common, significant discomfort usually arises when these structures are overstressed or injured.
Impact of Ligamentum Flavum Hypertrophy:
- Compression of spinal nerves.
- Reduction of spinal canal space.
- Chronic lower back discomfort and sciatica-like symptoms.
L4-L5 Slip-Disc (Slipped Disc)
A slipped disc at L4-L5 occurs when the spinal disc between the vertebrae deteriorates, bulges, or herniates, pressing against the nerves or spinal cord. The smallest compression of a nerve root at this level can lead to significant complications, including nerve degeneration, weakness, and paralysis.
Potential Causes:
- Repetitive strain or trauma to the lower back.
- Age-related degeneration of the intervertebral disc.
- Poor posture or improper lifting techniques.
Symptoms of a compressed nerve from a slipped disc may include:
- Radiating leg discomfort (sciatica).
- Numbness, tingling, or weakness in the lower limbs.
- Loss of bowel or bladder control in severe cases.
What Causes L4-L5 Disc Bulge and Slip Disc Problems
L4-L5 disc disorders often described as slip disc problems such as disc bulge, extrusions or herniation, usually develop gradually rather than from one single event. The L4-L5 disc is one of the busiest parts of the lower back because it handles frequent bending, sitting, lifting, and load transfer between the upper body and pelvis. Over time, repeated stress can affect how the disc, nearby joints, and surrounding muscles work together.
Long hours of sitting, commuting, driving, and working in fixed positions are common. These daily habits can place ongoing stress on the lower back, especially on the L4-L5 spinal segment, where movement and load are often high. Some people first notice stiffness after sitting, while others notice changes when standing, walking, bending, or changing position.
4 Common Factors Linked to L4-L5 Bulges, Prolapses & Protrusions
- Prolonged sitting and posture habits: Sitting for long periods with limited movement can increase stress on the lower back
- Repetitive bending or lifting: Frequent bending, lifting, or repeated strain may place added load on the disc and nearby joints
- Reduced muscle support: When the core, hip, and lower back muscles are not working well together, the spine may take on more load during movement
- Gradual disc wear over time: Age-related changes can affect disc structure, including hydration, flexibility, and load handling
Why L4-L5 Disc Prolapse, Bulge & Protrusions Matter Over Time
When these factors build up, the L4-L5 disc protrusion, bulge or prolpase may become less able to handle pressure well. Nearby joints and nerve pathways may also become more sensitive to movement and load. That is why some people notice symptoms that extend from the lower back into the buttock or leg.
Why Caution Matters With L4-L5 Disc Problems
If L4-L5 disc disorder such as disc bulge or herniation are already present, extra care is needed with repeated bending, twisting, or forceful back cracking. In Malaysia, some people may first try bonesetting or manual methods that are not based on detailed spinal assessment or imaging review. That can be a concern when leg symptoms, tingling, numbness, or weakness are already present.
For L4-L5 disc concerns, it is better to begin with proper assessment and with care guided by practitioners trained to evaluate disc, joint, and nerve involvement in a structured clinical way. Knowing what is present helps guide what may need more caution.
What This Means for Daily Activity
Paying attention to early changes in the L4-L5 spinal segment can help reduce repeated stress over time. Posture habits, movement patterns, and muscle coordination all matter. For people in KL and PJ, small daily patterns such as long sitting hours, limited breaks, repeated lifting, or sudden twisting can add up more than expected.
L4-L5 MRI and Diagnosis: When Imaging Is Needed
For L4-L5 disc concerns, understanding what is happening at the disc and surrounding structures helps guide the next steps. A physical assessment often looks at movement, posture, reflexes, leg strength, and how the spine responds to different positions.
When available, imaging such as MRI or X-ray may provide additional detail. These images can show how the disc, joints, and nearby nerve spaces are shaped, which helps clarify whether spinal disc damages such as disc bulge, herniation, or narrowing are present.
Combining physical findings with imaging helps build a clearer picture of how the L4-L5 level is functioning during daily activity and which findings may need more caution.
L4-L5 Disc Bulge vs Herniation: Why the Terms Sound Similar but May Not Mean the Same Thing
L4-L5 disc bulge and L4-L5 disc herniation are related terms, but they do not always describe the same degree or pattern of disc change. A disc bulge usually refers to a broader change in the disc outline, while a herniation usually refers to a more focal area where disc material extends farther than expected. On imaging, both may appear at the same spinal level, but the wording can suggest different shapes, different locations, and sometimes different effects on nearby nerve spaces.
That said, the wording on an MRI report does not always explain the whole clinical picture. A person with a bulge may have more symptoms than someone with a herniation, and a larger imaging finding does not always mean stronger symptoms. The more useful question is not just what the report calls it, but whether the disc change is affecting nearby joints, nerve pathways, walking tolerance, or daily activity.
This is why L4-L5 MRI and diagnosis should not rely on one term alone. The report wording matters, but symptoms, physical examination, leg findings, and movement tolerance matter just as much. In practical terms, the difference between a bulge and a herniation helps describe the shape of the disc change, but the decision-making still depends on the full picture.
Why the Difference Between Bulge & Herniation at L4-L5 Matters
- A bulge and a herniation may look different on MRI
- Either one may exist with or without major symptoms
- Either one may contribute to sciatica if nerve spaces are affected
- Report wording helps, but symptoms and examination guide the next step more clearly
Video: L4-L5 Disc Bulge vs Herniation — What the MRI Terms Mean
MRI reports often use words like disc bulge, herniation, protrusion, or slipped disc, but many readers are left unsure what those terms actually mean. This short video helps explain the difference between a bulging L4-L5 disc and an L4-L5 disc herniation, why the wording matters, and why symptoms do not always match the size of the finding on a scan.
Key Moments of Disc Herniation and Bulge Video
- 00:00 Intro to disc bulge, disc herniation, and slipped disc
- 00:35 What spinal discs do and how they handle load
- 01:10 Why disc damage begins before larger disc issues appear
- 01:28 How annular tears develop
- 01:45 Bulge versus herniation: which comes first and why
- 02:09 Bulge, herniation, and extrusion explained
- 02:43 Why disc location can affect sciatica and leg symptoms
Understanding Disc Damage: From Early Wear to Herniation and Fragmentation
Spinal disc damage usually develops in stages rather than all at once. Early disc wear may begin with dehydration, reduced disc height, or loss of flexibility. As the outer disc fibers weaken, the disc may begin to bulge, then progress to protrusion, prolapse, herniation, extrusion, or fragmentation. Each stage can affect the spine, nearby joints, and nerve spaces differently, which is why the symptoms and imaging findings may change over time.
The pages below explain the main stages of disc damage and how each one fits into the broader slipped disc process:
- Degenerative Disc Disease: Learn how early disc wear, dehydration, and reduced disc height may begin the damage cycle and change how the spine handles load.
- Where a Disc Bulge Fits in the Disc Damage Cycle: Understand how a disc bulge develops, how it differs from later stages, and why it may or may not affect nearby nerves.
- Disc Prolapse: Explore how prolapse fits within the progression of disc damage and why the disc may begin to extend farther into nearby spaces.
- Protruded Disc: See how a protruded disc differs from a bulge and how the shape and location of the disc change may influence symptoms.
- Ruptured Disc: Learn what happens when the outer disc fibers tear more clearly and how that stage may increase the chance of nerve irritation.
- Herniated Disc Care in Kuala Lumpur: Review the broader herniated disc page for an overview of symptoms, imaging, nerve involvement, and non-surgical care.
- Extruded Disc: Understand how extrusion differs from earlier stages and why more advanced disc displacement may change symptoms or MRI findings.
- Fragmented and Sequestered Disc: Learn about the later stages of disc damage, where disc material may separate further and affect nearby nerve spaces in different ways.
Taken together, these pages explain how disc damage can progress from early degeneration to more advanced slipped disc stages, and why accurate imaging, symptom patterns, and careful assessment matter at every step.
Why Twisting and Forceful Back Cracking May Need More Caution With L4-L5 Disc Problems
L4-L5 disc bulge and herniation can make the lower back less tolerant of repeated twisting, forceful rotation, and self-cracking. When disc damage is already present, the outer disc fibers and nearby tissues may be less able to handle sudden rotational load. That matters because L4-L5 is one of the busiest parts of the lower back during sitting, bending, lifting, and daily movement.
For people with L4-L5 leg symptoms, tingling, numbness, or weakness, caution becomes even more important. A careful review of symptoms, physical findings, and imaging may help guide which hands-on methods may need more caution and which movements may be better avoided. The goal is not to create fear. The goal is to recognize that disc-related problems are not all the same, and forceful twisting or cracking may not suit every L4-L5 presentation.
Published discussion on disc herniation and manipulation has also emphasized risk-reward thinking, especially when an L4-L5 herniated disc is suspected or already confirmed. That is why L4-L5 care is often better guided by assessment first, then by gentle and focused methods that match the person’s findings rather than by generalized forceful rotation.
Reference for forceful back care:
- Erwin WM. Should you adjust that herniated disc? Thoughts from a chiropractor/molecular scientist. J Can Chiropr Assoc. 2023;67(1):7-18.
Activator Method for L4-L5 Disc Bulge: Why a Low-Force, Non-Twisting Approach May Be Considered
For a bulging L4-L5 disc and L4-L5 disc herniation, the Activator Method is often considered when a lower-force, non-twisting approach is preferred. The instrument delivers a quick, controlled impulse in a more neutral setup, which may matter when the disc, nearby joints, or nerve pathways are less tolerant of added rotation or strong manual force. In disc-related cases, that mechanical difference is often part of the safety discussion.
Published research does not clearly prove that the Activator Method produces better final outcomes than manual high-velocity, low-amplitude methods across all low back cases. The broader review literature instead reports comparable clinically meaningful benefits, while also noting that the available studies have important limitations such as small sample sizes, brief follow-up, and limited controls.
Where the Activator Method may stand out for L4-L5 slip disc care is in its mechanical profile. The case report you provided discussed possible benefits for symptomatic lumbar disc herniation because the instrument-assisted method avoids the torsional stress commonly associated with side-posture setups, and the authors specifically called for further study on the safest and most effective way to manage disc lesions in a chiropractic setting. That makes it reasonable to describe Activator as a method that may be better suited for some L4-L5 disc presentations, especially when safety and reduced twisting are top priorities.
For people with L4-L5 leg symptoms, tingling, numbness, weakness, or disc findings on MRI, the key question is not which method sounds stronger. The better question is which method places less unwanted stress on the involved structures while matching the person’s exam findings. For that reason, technique choice is usually strongest when it follows assessment first, then a method that fits the disc, joint, and nerve presentation.
Research References for Activator Method and L4-L5 Disc Herniation
- Polkinghorn BS, Colloca CJ. Treatment of symptomatic lumbar disc herniation using activator methods chiropractic technique. J Manipulative Physiol Ther. 1998;21(3):187-196.
- Huggins T, Boras AL, Gleberzon BJ, Popescu M, Bahry LA. Clinical effectiveness of the activator adjusting instrument in the management of musculoskeletal disorders: a systematic review of the literature. J Can Chiropr Assoc. 2012;56(1):49-57.
L4-L5 Spondylolisthesis: Symptoms, Grades, and What It Means
L4-L5 spondylolisthesis means the L4 vertebra has shifted forward in relation to L5. At this level, that shift can change how the lower back, pelvis, sacrum, discs, and nearby nerve spaces handle daily load. Some people notice lower back stiffness, while others notice leg symptoms, walking issues (leg weakness), or reduced tolerance for sitting and standing.
L4-L5 spondylolisthesis is commonly described by grade, based on how far the vertebra has shifted forward:
- Grade 1: up to 25% slip
- Grade 2: 26% to 50% slip
- Grade 3: 51% to 75% slip
- Grade 4: more than 75% slip
The grade is important, but the grade alone does not explain the whole condition. Slip disc, nerve involvement, pelvic alignment, walking tolerance, muscle control, and imaging findings all matter when deciding what kind of care may fit better. That is why two people with the same grade may still need different approaches.
For a broader explanation of causes, grading, and long-term planning, readers can visit the main spondylolisthesis page.
Why L4-L5 Spondylolisthesis Care Often Needs More Stability and Less Force
Spondylolisthesis care for the L4-L5 or the L5-S1 is usually not approached like an ordinary stiff lower back. When one segment has shifted forward, the main concern is not simply increasing motion. The priority is improving how the lower back, pelvis, and nearby segments handle load without adding unnecessary shear, twisting, or force to the slipped level.
That is why stability often comes first. When the spinal disc protrudes, bulges or ruptures, nerve symptoms, pelvic imbalance, or segmental irritation are present, lower-force and position-based methods may be more appropriate than generalized rotational methods. The question is not which method feels strongest. The better question is which method places less unwanted stress on the involved segment while improving control above, below, and around it.
Methods Commonly Used for L4-L5 Spondylolisthesis Care & Those for L5-S1
For L4-L5 spondylolisthesis, care is often structured in three parts: stability-focused methods, disc-pressure management methods, and supportive rehabilitation methods.
- Stability-Focused Methods: Lower-force methods may be chosen when the slipped segment is less tolerant of twisting or forceful manual setups.
- SOT pelvic blocking: Used to influence pelvic balance and lumbosacral positioning in a lower-force way
- Activator Methods: A low-force, instrument-assisted approach that can be used when a more controlled, non-twisting setup is preferred
- Disc-Pressure Management Methods of L4-L5: When disc damage and slippages are also present, some methods may be selected to reduce compressive load and improve how the lower back handles movement.
- Flexion-distraction: Often considered when the goal is to reduce pressure while improving movement in a more controlled setup
- Non-surgical spinal decompression: In selected cases, decompression-based care may be used as part of a broader plan focused on disc-related load management
- Supportive Rehabilitation Methods of Lower Back L4-L5 and L5-S1: These methods are often used to improve tolerance, movement control, and daily function around the involved segment.
- Guided rehabilitation and stabilization exercise: Used to improve control through the core, pelvis, and lower back
- Therapeutic ultrasound: May be included as part of supportive soft-tissue care
- Electrotherapy: May be used in the lumbar or sacral region as part of a broader plan focused on comfort and muscle guarding
- High-intensity laser therapy: May be considered as an adjunct in musculoskeletal care plans.
- hockwave therapy: May also be used in selected cases as part of supportive soft-tissue and rehabilitation-based care
The key point is that L4-L5 spondylolisthesis treatment plans should follow the findings. Technique choice should be based on imaging, symptoms, physical examination, and how the lower back responds to load during daily activity.
L4-L5 Spondylolisthesis Care References
- Adar S, Apaydın O, Dündar U, et al. Comparison of the Effectiveness of Traditional Motorized Traction and Non-surgical Spinal Decompression Therapy Added to Conventional Physiotherapy for Treatment of Chronic Low Back Pain. Cureus.2024;16(9):e69610. Published 2024 Sep 17. doi:10.7759/cureus.69610.
- Song HJ, Seo HJ, Lee Y, Kim SK. Effectiveness of high-intensity laser therapy in the treatment of musculoskeletal disorders: A systematic review and meta-analysis of randomized controlled trials. Medicine (Baltimore).2018;97(51):e13126. doi:10.1097/MD.0000000000013126.
- Walewicz K, Taradaj J, Dobrzyński M, et al. Effect of Radial Extracorporeal Shock Wave Therapy on Pain Intensity, Functional Efficiency, and Postural Control Parameters in Patients with Chronic Low Back Pain: A Randomized Clinical Trial. J Clin Med. 2020;9(2):568. Published 2020 Feb 19. doi:10.3390/jcm9020568.
L4-L5 Facet Hypertrophy and Ligamentum Flavum Thickening: Why They Often Develop Together
At the L4-L5 level, facet hypertrophy and ligamentum flavum thickening often develop together rather than as isolated findings. The facet joints, their capsular ligaments, and the ligamentum flavum are closely related parts of the same motion segment. Over time, repeated loading, prolonged sitting, poor posture, injuries, and age-related wear can change how that segment handles pressure and motion. As the facet joints become more stressed, the articular cartilage may lose its smooth structure and the surrounding soft tissues may adapt by becoming thicker, stiffer, or less flexible.
This is one reason L4-L5 spinal stenosis often does not come from one structure alone. In many cases, the crowded space is created by a combination of facet overgrowth, ligament thickening, bulges, herniations, and disc prolapses , and sometimes spondylolisthesis. When that happens, the canal or nearby nerve spaces may become narrower, which can affect the lower back, buttock, thigh, or leg. Older MRI studies and current clinical practice both support the idea that these changes often occur together rather than separately.
L4-L5 Spinal Stenosis: Why Disc Problems, Facet Overgrowth, and Ligament Thickening Can Narrow the Space
L4-L5 spinal stenosis means the space available for the nerves becomes narrower at the L4-L5 level. This narrowing may happen in the central canal, the lateral recess, or the foraminal space, and each pattern can affect symptoms differently. At L4-L5, stenosis often develops gradually through degenerative changes rather than from one single structure alone. Common contributors include disc bulge, facet hypertrophy, osteophyte formation, ligamentum flavum thickening, and sometimes degenerative spondylolisthesis. StatPearls also notes that L4-L5 is the most commonly affected level for lumbar spinal stenosis.
As the available space narrows, nearby nerve structures may become crowded. That is one reason some people notice leg heaviness, tingling, numbness, walking limitation, or symptoms that increase with standing and lumbar extension. Forward bending may feel easier for some people because flexion can temporarily create a little more space, which is why walking uphill or leaning forward on a shopping cart may feel better than standing upright for long periods. Severe cases may involve motor weakness, gait changes, abnormal postural sway, or bowel and bladder changes, which need faster medical attention.
MRI is often the most useful imaging test when L4-L5 stenosis is suspected because it helps show whether the narrowing is coming more from the disc, the facets, the ligamentum flavum, or a combination of all three. The imaging matters, but the symptoms and physical findings matter just as much. StatPearls also emphasizes that severe-looking canal narrowing on MRI does not always match the symptom level, so the full picture is more important than one measurement alone.
Reference for L4-L5 Spinal Stenosis
- Munakomi S, Cruz R. Lumbar Spinal Stenosis. StatPearls [Internet]. Updated January 30, 2024. StatPearls Publishing; 2026 Jan-.
How These Changes Can Affect the Canal and the Legs
When the L4-L5 canal becomes crowded, symptoms may shift beyond the lower back. Some people notice leg heaviness, tingling, numbness, or changes in walking tolerance. Others notice symptoms during standing or walking that improve somewhat with sitting or bending forward. This pattern matters because it suggests that the problem may involve more than a single painful joint. It may reflect pressure or crowding around the nerve spaces, especially when facet hypertrophy, ligamentum flavum thickening, and disc-related changes are present together.
Why Forceful Twisting and Repeated Cracking May Need More Caution at L4-L5
A hypertrophic L4-L5 facet joint does not behave like a normal, healthy, freely moving joint. When the facet capsule is thickened, the ligamentum flavum is less flexible, and the surrounding segment is already crowded, forceful twisting or repeated cracking may place additional stress on a segment that is already less tolerant of rotation and shear.
That does not mean all hands-on care is inappropriate. It means the L4-L5 segment should not be treated like an ordinary stiff lower back. The more useful question is whether a method adds unwanted force to an already crowded segment, especially when leg symptoms, numbness, tingling, weakness, or walking intolerance are already present. In these cases, proper assessment matters first. That is the safest starting point. This same safety-first logic is consistent with the way disc-related and nerve-related cases are approached elsewhere in the literature you shared.
References for L4-L5 Facet Hypertrophy and Ligamentum Flavum Thickening
- Adar S, Apaydın O, Dündar U, et al. Comparison of the Effectiveness of Traditional Motorized Traction and Non-surgical Spinal Decompression Therapy Added to Conventional Physiotherapy for Treatment of Chronic Low Back Pain. Cureus. 2024;16(9):e69610.
L4-L5 Facet Joint RFA and Surgery: What the Research Says
When L4-L5 facet hypertrophy and ligament thickening are already narrowing the space, some people are offered surgery or radiofrequency ablation (RFA). The problem is that these options do not answer the same question.
Surgery may create more room, but it also changes the mechanics of the segment. RFA works differently. It aims to interrupt pain signaling from the targeted nerves, but it does not directly change the underlying crowding, the thickened ligament, the enlarged facet, or the way the segment handles load. That is why a patient may still need a careful stability-focused plan even after the procedure.
The strongest study you shared on RFA is the Mint randomized clinical trials. In those trials, radiofrequency denervation combined with a standardized exercise program resulted in either no improvement or no clinically important improvement compared with the standardized exercise program alone for chronic low back pain arising from the facet joints, sacroiliac joints, or combined sources. The authors concluded that the findings did not support the use of radiofrequency denervation for chronic low back pain from those sources.
That does not mean every patient has the same experience. It does mean that the research is not as supportive as many people assume, especially when the underlying issue is structural crowding at L4-L5 rather than a simple isolated pain signal.
Conservative-First Reasoning for a Crowded L4-L5 Segment
For a crowded L4-L5 segment, the conservative-first discussion is not just about symptom control. It is also about preserving how the segment, pelvis, and nearby stabilizing tissues handle load over time. When facet hypertrophy, ligamentum flavum thickening, disc changes, and sometimes spondylolisthesis are present together, the long-term question becomes larger than short-term symptom reduction. It becomes a question of whether the next step improves function without adding more instability, more crowding, or more dependence on repeat procedures.
That is why many patients first need a clear explanation of what is actually causing the crowding and which findings matter most on imaging and physical examination. Once that is clear, the discussion about options becomes much more useful.
References for L4-L5 Facet Joint RFA and Surgery
- Juch JNS, Maas ET, Ostelo RWJG, et al. Effect of Radiofrequency Denervation on Pain Intensity Among Patients With Chronic Low Back Pain: The Mint Randomized Clinical Trials. JAMA. 2017;318(1):68-81.
Supportive Non-Surgical Measures Sometimes Used Around L4-L5
When the L4-L5 segment is crowded by facet hypertrophy, ligament thickening, and related degenerative changes, supportive non-surgical measures are often discussed as part of a broader plan rather than as stand-alone answers.
The studies you shared suggest that adding traction or spinal decompression to conventional physiotherapy may improve pain and disability more than conventional physiotherapy alone in selected lumbar discopathy groups, although spinal decompression did not clearly outperform conventional motorized traction in that study.
The high-intensity laser review you shared reported significant improvements in pain and disability scores compared with controls across musculoskeletal disorders, including back pain, while also noting moderate risk of bias and the need for better long-term studies.
The shockwave trial you shared found better results for pain, function, and postural control than the comparison group in chronic low back pain, especially during follow-up.
These findings do not prove that any single method is the answer for facet hypertrophy or ligamentum flavum thickening. What they do support is the idea that a supportive, conservative-first discussion is reasonable, especially before jumping straight to more invasive options.
References for Supportive Non-Surgical Measures Around L4-L5
- Adar S, Apaydın O, Dündar U, et al. Comparison of the Effectiveness of Traditional Motorized Traction and Non-surgical Spinal Decompression Therapy Added to Conventional Physiotherapy for Treatment of Chronic Low Back Pain. Cureus. 2024;16(9):e69610.
- Song HJ, Seo HJ, Lee Y, Kim SK. Effectiveness of high-intensity laser therapy in the treatment of musculoskeletal disorders: A systematic review and meta-analysis of randomized controlled trials. Medicine (Baltimore). 2018;97(51):e13126.
- Walewicz K, Taradaj J, Dobrzyński M, et al. Effect of Radial Extracorporeal Shock Wave Therapy on Pain Intensity, Functional Efficiency, and Postural Control Parameters in Patients with Chronic
Video: Why L4-L5 Back and Leg Issues Keep Coming Back
Many L4-L5 back and leg issues improve for a while, then return again. That pattern is often linked to incomplete assessment, short-term patching, or failure to identify all the structures involved. In this video, Yama Zafer explains why recurring lower back, disc, joint, and nerve issues are common and why long-term decisions should be based on the full mechanical and clinical picture.
Key Moments for Video on Recurrent Back Issues
- 00:00 Why neck and back problems often return
- 00:25 Why short-lived improvement does not always mean full recovery
- 01:00 How shortcuts can lead to recurrence
- 02:05 Why identifying the real drivers matters
- 02:35 Single-factor care versus multifaceted care
- 03:00 Why informed decisions matter before choosing the next step
Recap: What Matters Most for L4-L5 Disc Issues, Sciatica, Stenosis, and Nerve-Related Changes
L4-L5 disc problems are often not caused by one structure alone. A disc bulge or herniation at L4-L5 may appear together with sciatica, nerve compression, facet hypertrophy, ligamentum flavum thickening, spinal stenosis, or spondylolisthesis. When these changes develop at the same time, the result may be more than lower back discomfort. The buttock, thigh, calf, foot, walking tolerance, balance, and leg control may also be affected.
That is why L4-L5 care should not begin with guesswork, routine force, or a one-size-fits-all plan. The more useful starting point is to understand what the imaging shows, how the symptoms behave, and whether the main issue is disc-related stress, nerve irritation, canal narrowing, segmental instability, or a combination of these. MRI findings matter, but symptoms, walking changes, neurologic findings, and daily load tolerance matter just as much.
This page also explains an important point many people are not told early enough: not every modern-sounding procedure is strongly supported for long-term benefit, and not every hands-on method suits a crowded or unstable L4-L5 segment. When symptoms include tingling, numbness, weakness, sciatica, foot drop, walking intolerance, or imaging-confirmed narrowing, the safer path is usually the one guided by findings, caution, and structure rather than routine force or quick fixes.
For readers in Kuala Lumpur and Petaling Jaya, the key message is simple: when L4-L5 symptoms affect the leg, foot, walking, or daily function, a careful assessment-first plan is often the most useful way to decide what needs attention first, what may need more caution, and which next step makes the most sense.
Peer Reviewed References for L4-L5 Slip Disc, Sciatica, Stenosis, and Related Nerve Changes
- Sima S, Diwan A. Contemporary clinical perspectives on chronic low back pain: The biology, mechanics, etc. underpinning clinical and radiological evaluation. JOR Spine. 2025;8(1):e70021. Published 2025 Jan 23. doi:10.1002/jsp2.70021.
- Erwin WM. Should you adjust that herniated disc? Thoughts from a chiropractor/molecular scientist. J Can Chiropr Assoc. 2023;67(1):7-18.
- Polkinghorn BS, Colloca CJ. Treatment of symptomatic lumbar disc herniation using activator methods chiropractic technique. J Manipulative Physiol Ther. 1998;21(3):187-196.
- Huggins T, Boras AL, Gleberzon BJ, Popescu M, Bahry LA. Clinical effectiveness of the activator adjusting instrument in the management of musculoskeletal disorders: a systematic review of the literature. J Can Chiropr Assoc. 2012;56(1):49-57.
- Adar S, Apaydın O, Dündar U, et al. Comparison of the Effectiveness of Traditional Motorized Traction and Non-surgical Spinal Decompression Therapy Added to Conventional Physiotherapy for Treatment of Chronic Low Back Pain. Cureus. 2024;16(9):e69610. Published 2024 Sep 17. doi:10.7759/cureus.69610.
- Song HJ, Seo HJ, Lee Y, Kim SK. Effectiveness of high-intensity laser therapy in the treatment of musculoskeletal disorders: A systematic review and meta-analysis of randomized controlled trials. Medicine (Baltimore).2018;97(51):e13126. doi:10.1097/MD.0000000000013126.
- Walewicz K, Taradaj J, Dobrzyński M, et al. Effect of Radial Extracorporeal Shock Wave Therapy on Pain Intensity, Functional Efficiency, and Postural Control Parameters in Patients with Chronic Low Back Pain: A Randomized Clinical Trial. J Clin Med. 2020;9(2):568. Published 2020 Feb 19. doi:10.3390/jcm9020568.
- Munakomi S, Cruz R. Lumbar Spinal Stenosis. StatPearls [Internet]. Updated January 30, 2024. Treasure Island (FL): StatPearls Publishing; 2026 Jan-.
- Juch JNS, Maas ET, Ostelo RWJG, et al. Effect of Radiofrequency Denervation on Pain Intensity Among Patients With Chronic Low Back Pain: The Mint Randomized Clinical Trials. JAMA. 2017;318(1):68-81.
Author
Yama Zafer, D.C., author of L4-L5 Back Issues: Slip Disc, Sciatica & Stenosis | 7 Signs, trained in physiotherapy and chiropractic at Cleveland Chiropractic University in Kansas City, brings nearly 30 years of experience; read more about Y. Zafer.
Last updated
L4-L5 Disc Care Without Surgery in KL & PJ was significantly updated on April 21, 2026.
L4-L5 Back Issues FAQ: Slip Disc, Sciatica, Stenosis, MRI, and Nerve Symptoms
These FAQs cover common questions about L4-L5 back issues, including slip disc, sciatica, stenosis, nerve compression, MRI findings, foot drop, facet hypertrophy, ligamentum flavum thickening, and spondylolisthesis. The answers are written to help readers understand what the terms mean, how symptoms may develop, and when careful assessment matters more.
What are L4-L5 back issues?
L4-L5 back issues are lower back problems involving the disc, joints, ligaments, or nerve spaces between the L4 and L5 vertebrae. Common findings include disc bulge, herniation, sciatica, stenosis, facet hypertrophy, ligamentum flavum thickening, and spondylolisthesis.
What is an L4-L5 slip disc?
An L4-L5 slip disc usually refers to disc changes such as a bulge, protrusion, herniation, or extrusion at the L4-L5 level. These changes may or may not affect nearby nerves.
Is sciatica the same as an L4-L5 slip disc?
No. Sciatica is a symptom pattern, not a diagnosis by itself. An L4-L5 slip disc is one possible spinal cause of sciatica.
Can an L4-L5 disc bulge cause sciatica?
Yes. An L4-L5 disc bulge may contribute to sciatica if it irritates or crowds nearby nerve structures.
What is L4-L5 nerve compression?
L4-L5 nerve compression means nearby nerve tissue is being irritated, compressed, inflamed, or affected by a combination of these factors.
What is L4-L5 spinal stenosis?
L4-L5 spinal stenosis means the available space for the nerves becomes narrower at the L4-L5 level. This may happen in the central canal, lateral recess, or foraminal space.
Is L4-L5 the most common level for lumbar spinal stenosis?
Yes. L4-L5 is commonly described as the most frequently affected lumbar level for degenerative spinal stenosis.
What symptoms can L4-L5 problems cause?
L4-L5 problems may cause lower back stiffness, buttock symptoms, thigh or calf sensations, sciatica, numbness, tingling, weakness, walking changes, or reduced tolerance for sitting and standing.
What is the difference between an L4-L5 disc bulge and an L4-L5 disc herniation?
A disc bulge is usually a broader change in the disc outline. A disc herniation is usually a more focal extension of disc material. Either one may or may not cause symptoms.
Can L4-L5 problems cause numbness in the foot?
Yes. L4-L5 nerve compression may affect sensation in the outer leg, top of the foot, or big toe region.
Can L4-L5 problems cause foot drop?
Yes. L4-L5 foot drop may happen when nerve involvement affects foot lift or great toe lift. That kind of weakness needs faster medical assessment.
Why does tingling happen with L4-L5 nerve irritation?
Tingling often happens when the nerve is irritated or its signaling becomes unstable. It may feel like pins and needles, prickling, burning, or an electric-like sensation into the leg or foot.
Why does weakness happen with L4-L5 nerve compression?
Weakness may happen when motor nerve fibers are affected enough to reduce normal signal flow to the muscles. At L4-L5, this may influence foot lift, toe lift, or heel walking.
Do all L4-L5 MRI findings cause symptoms?
No. MRI findings and symptoms do not always match perfectly. That is why imaging should be read together with the history, physical examination, and neurologic findings.
Do I always need an MRI for L4-L5 symptoms?
Not always. MRI is often more useful when leg symptoms, nerve-related findings, weakness, or canal narrowing are suspected, or when symptoms are not improving as expected.
What is facet hypertrophy at L4-L5?
Facet hypertrophy means the facet joints at L4-L5 have enlarged or changed over time, often as part of degenerative wear and increased loading.
What is ligamentum flavum thickening at L4-L5?
Ligamentum flavum thickening means the ligament between adjacent laminae has become thicker or less flexible over time, which may contribute to canal crowding.
Can facet hypertrophy and ligamentum flavum thickening happen together?
Yes. They often develop together as part of the same L4-L5 motion segment changes.
Can facet hypertrophy and ligamentum flavum thickening affect the legs?
Yes. When they narrow the canal or nearby nerve spaces, they may contribute to tingling, numbness, heaviness, walking intolerance, or sciatica-like symptoms.
What is L4-L5 spondylolisthesis?
L4-L5 spondylolisthesis means L4 has shifted forward in relation to L5. This may change how the lower back, pelvis, discs, and nerve spaces handle load.
Does the grade of spondylolisthesis always match symptom severity?
No. The grade matters, but symptoms, nerve findings, walking tolerance, imaging, and overall stability matter too.
Can forceful twisting or repeated back cracking make L4-L5 problems worse?
It may need more caution, especially when disc changes, nerve symptoms, facet overgrowth, ligament thickening, or instability are already present.
Can L4-L5 symptoms improve without surgery?
Yes. Many people first consider a conservative-first approach, especially when there is no urgent neurologic decline.
When should L4-L5 symptoms be assessed more urgently?
Faster medical assessment is important when there is worsening weakness, foot drop, major walking changes, bowel or bladder changes, or rapid neurologic decline.



What is the cost for L4-L5 Slip-Disc treatment?
Thank you for your question. Fees for L4-L5 slip disc care depend on the MRI findings and whether the problem involves a disc bulge, protrusion, herniation, extrusion, joint problem, or nerve compression. Exact costs are discussed after assessment. For current fees and appointment details, please contact our center directly.
My MRI shows my intervertebral disc heights at:
L1-L2 at 11 mm
L2-L3 at 7.2mm
L3-L4 at 1mm
L4-L5 at 6.8mm
L5-S1 at 13 mm.
I can walk up to one minute. I have been suffering from this problem for the last 20 years. Please suggest what I should do now. I am residing in India.
Dear Raghubir,
I suspect you have severe spinal canal stenosis from multilevel spinal disc, spinal joint, and ligamentous issues combined. From what i understand, there are no effective non-surgical treatment options in India for patients with degenerative disc disease, bulging discs, or herniated discs that cause spinal canal stenosis. Moreover, there is nothing that I can tell you that you could do to make it feel better.
would be best to have advanced non-surgical spine care, preferably through NSD Therapy® methods combining chiropractic and physiotherapy. In India, many claim to be a chiropractor without having a chiropractic degree from an accredited Univiserty. Alternatively, you can visit our center in Kuala Lumpur, Malaysia. FOr more information, please WhatsApp us when ready.
Hi Do they have this care in San Diego and do they take Anthem bluecross Medicare
Dear Kathy,
We are currently in Malaysia, but we hope to one day be in the United States.
Hi Mychiro,
Do you need an MRI to get treatment for the l4-l5 slip disc? My case is severe; how many sessions and how long will it take to complete the treatment? I really appreciate any help you can provide.
Dear Raghubir,
Based on what you shared, your MRI appears to show multilevel disc and joint degeneration, with very advanced narrowing at L3-L4 and additional disc height loss at L4-L5. Walking tolerance limited to about one minute can happen when the lower back is dealing with significant canal or nerve-space narrowing. Because of that, the next step should be a careful review by a qualified spine clinician who can examine you in person and correlate your symptoms with the MRI.
When walking becomes that limited, the main priority is to determine whether the problem is affecting the nerves, walking function, or spinal stability more seriously. Since I cannot assess you directly here, it would be safer to seek an in-person spine evaluation with your MRI films and report available for review. If you are considering care with our center, please contact us directly for appointment information.
My problem is related to a disc issue causing sciatica pain that I believe is coming from L1-L2, L3-L4.and L5-S1.
Dear Dhoni,
Sciatica arises when the lower back nerve impingement or compressed. The compression can result from bone spurs, slipped discs, ligamentous or muscle issues. To recover, you will need to have the root cause identified and corrected. We have treated thousands of patients with sciatic issues without the need for medication, injections, or surgery. Our integrative methods of care combine chiropractic and physiotherapy. Moreover, the care we provide for sciatica patients is enriched with advanced therapy devices such as RxDecom, High-Intensity Laser Therapy, shockwave therapy, in addition to general physiotherapy and chiropractic therapy devices. Learn more about our sciatica treatment by calling us on 03 2093 1000.
Hi sir
My name is Dinakar, and I am 48yr old. I have problems with L4 and L5 slip disks issue. My surgeon recommends another spine surgery. My last spine surgery was in 1997 for the same problem. Please suggest what I do, my financial condition is awful, I lose my job when—Covid 2nd wave. Please suggest me.
Thanks and regards
Dinakar
Dear Mr. Dinakar,
Thanks for posting a question. Spine surgery should always be the last option, as they often fail or need further surgical interventions.f It is not uncommon for a person to have more than one surgical intervention. Some have even had two or more spine surgeries and still live with pain.
As far as your current condition, I would encourage you to seek conservative measures before your second surgery. The first step is to thoroughly assess your spine to see how our methods can help. We will need to review your previous MRI and X-ray scan as well.
I understand your plight with financial issues; however, patients who experience back pains after having surgery require attentive care. As such, there is little that you can do to solve the problem. In short, you need focused treatments that focus on damaged tissues for lasting relief. Should you need our help, please contact our office on 03 2093 1000.
I greatly appreciate your help with my spinal injuries I have herniated disc. How can I access you?
Dear Jerusha< We have helped thousands recover from a herniated disc without surgery or injections. Our advanced methodology, combined with breakthrough spine technology, can help. We have an award-wing team of physiotherapists and Malaysia’s best chiropractor to help patients like you. Please feel free to contact our center via WhatsApp for additional information.
We look forward to hearing from you soon.
I am suffering from an L4-L5 spinal stenosis and have a foot drop in my left leg, with neurogenic claudication. Please tell me what I can do. I am from India।
Thank you for reaching out about your condition involving L4-L5 spinal stenosis and the associated foot drop in your left leg, along with neurogenic claudication. This is a complex issue but one that we frequently address with considerable success through a tailored approach to rehabilitation.
Spinal canal stenosis, especially at the L4-L5 and L5-S1 levels, can result from various factors, including hypertrophy of the facet joints, thickening of the ligamentum flavum, spinal disc bulges, degenerative arthritis, and occasionally spondylolisthesis. These factors often occur simultaneously and contribute to the narrowing of the spinal canal, which in turn causes the symptoms you are experiencing.
Treatment Options: Our clinic specializes in non-surgical treatments that are highly effective for conditions like yours. These include:
• Non-rotatory Chiropractic Care: Specifically tailored for spinal canal stenosis to relieve pressure without aggressive manipulation.
• Spinal Decompression Therapy: This method gently stretches the spine, which can help relieve pressure on compressed nerve roots and reduce symptoms of stenosis.
• Physiotherapy: Customized therapies by specialized machines and hands-on physiotherapy designed to repair damaged tissue and stabilize the lower back and pelvis.
• Rehabilitation: Integrative approaches that focus on long-term health and pain management.
Regarding Neurogenic Claudication: This condition, characterized by pain and cramping in the legs due to spinal stenosis, can significantly benefit from our specialized methods. Our therapies are designed to improve blood flow, reduce nerve irritation, and enhance mobility, which can alleviate the symptoms of claudication.
If you want to learn more about how our treatments can specifically help with your spinal stenosis and associated symptoms, or if you wish to schedule a consultation, please contact us via WhatsApp at +(60)17-269-1873. We understand your challenges, and our goal is to help you achieve better health and improved quality of life without the need for invasive procedures.We look forward to the opportunity to assist you.
Best regards,
I have an L4 L5 and L5 S1 disc disease, can you help?
Dear Sanchita,
Thanks for posting a question. Our center is the premier non-surgical treatment center for neck pain, back pain, sciatica, and slipped disc. Our advanced mythologies and specialized therapy devices have helped thousands recover. I am confident that we can do the same for you. Watch this short video on our slipped disc treatment. It will help you understand how we treat patients with disc disorders. Should you wish to set an appointment for your initial consultation, please call our main center at 03 2093 1000. We have several centers in the Klang Valley.
Hope this helps
I have a problem with my L4 L5. I now experience nerve pain due to spinal nerve compression in my left leg. Can this be helped?
Dear Sham,
Chiropractic Specialty Center® is Malaysia’s premier non-surgical spine and joint center. The most common cause of pain, numbness, tingling, and weakness in the legs is nerve compressions at L4-L5 or L5-S1. Slipped discs such as bulging, protruded, prolapsed, herniated, and extruded discs are the leading causes of back and leg pain that cause sciatica-like symptoms. Our methods of treating leg pain slipped discs, and back pain is through advanced evidence-based practices of chiropractic combined with physiotherapy. Our clinical team’s chiropractic and physiotherapy treatment include sophisticated therapy devices targeting the root causes of back and leg pains, including sciatica and sciatica-like nerve symptoms.
I have the same symptoms. My doctor is requesting surgery because I have done a one-month recovery program, and my leg pain has lasted almost two years. Could you provide me with advice if I provide my MRI result?
Dear Eric,
I am sorry, but I do not provide consultation or review medical records of patients in pain for diagnosis and treatment advice. However, I would happily assess you in my office if you book an appointment. This is the best way to eliminate mistakes and provide the best non-surgical options; please WhatsApp our center to book a consultation.
Compression L3 and L4 and L5
Thank you for sharing your concerns about compression at your spine’s L3, L4, and L5 levels. This condition can lead to discomfort and other symptoms affecting your lower back and legs.
At CSC, we recommend consulting with one of our experienced chiropractors who specializes in holistic, non-invasive treatments. These methods are designed to alleviate your symptoms effectively while addressing the root cause of the compression. Our approach includes targeted physical therapy, personalized rehabilitation plans, and advanced non-surgical techniques, providing comprehensive spine care that aims for a faster recovery with lasting benefits.
To manage your condition effectively:
• Schedule a Consultation: Discuss your symptoms in detail with our chiropractic team to get a tailored treatment plan.
• Engage with CS’s Customized chiropractic, spinal decompression, flexion-distraction therapy, physiotherapy, and rehabilitation to repair damaged tissue, strengthen supportive muscles, and enhance spinal health through personalized exercises.
• Adopt Healthy Lifestyle Adjustments: Make ergonomic improvements and lifestyle changes to support your spine health.
Please feel free to WhatsApp us for more information at (60)17-269-1873 or to schedule an appointment. We’re here to help you achieve optimal health and improve your quality of life.
Best regards
Would you know anyone you can refer me to in Southern California, USA?
Dear Barbara,
Unfortunately, we are not aware of anyone in California that offers comprehensive and integrative methods of spine care through chiropractic and physical therapy. I encourage you to call some center in the neighborhood and ask if they provide comprehensive physical therapy combined with chiropractic.
I have a problem with L3-L4, l-l5, and L5-S1. The spinal canal dimensions are 9.3 and 9.8 mm, respectively, with the most recent MRI. I have undergone three sitting of Chiropractic, but the problem is not resolved. Further, the chiropractor asked for guidance from Neurosurgeon. I have radiating pain in the buttock, thigh, and right leg when walking. I could walk for 4 KM without pain in the past, but now everything has changed. Also, at present, I am undergoing IFT in a physiotherapy center.
Please advise what to do?
Dear Mr. Vijay,
Thanks for posting your question. L3-L4 and L4-L5 problems are common back-related issues that impact millions. Based on what you have related, you also suffer from spinal canal stenosis. And as such, there may be additional findings present in your MRI assessment. Other issues such as facet hypertrophy and ligamentum flavum hypertrophies are expected when the L3-L4 and L4-L5 spinal segments cause canal stenosis.
Also, you mentioned that you had received chiropractic treatment and IFT (electrotherapy) from a physiotherapy center. Chiropractic treatment alone will not make much of a difference with this level of damage. And IFT as a standalone therapy is a waste of time.
To recover, you will require focused therapies that incorporate chiropractic treatment spinal disc methods combined with slipped-disc-specific physiotherapy methods.
At Chiropractic Specialty Center®, we provide NSD Therapy®. NSD Therapy® services is the most advanced form of non-surgical spine care, specific to patients like you. I am a chiropractor who has treated patients like you successfully for over 25-years, and I am confident that we can provide you with the precision treatment needed to help your recovery.
Please get in touch with our main center on 03 2093 1000 or WhatsApp us to schedule a detailed assessment or for more information about our methods of care. Please ask to be seen by Dr. Yama (that’s me).
I hope this helped.
I have an L3-L4 right paracentral disc protrusion with severe stenosis of the right lateral recesses. Is this treatable without surgery?
Dear Mohammad,
Thanks for posting a question, and please forgive us for replying to you late. An L3-L4 disc protrusion is treatable without surgery. NSD Therapy® is the best non-surgical method of care. It incorporates disc-specific chiropractic, physiotherapy, and rehabilitation methods during the same session. Treatments are personalized to the needs of patients and non-painful. Over the years, we have helped thousands recover with a 95% success rate. Contact us today for more information about the best chiropractic and top-rated physiotherapy treatment you can get from a slipped disc. You may call or WhatsApp us when ready. I hope this helped.
My question. I’m 71 years old with heart and kidney disease. My L4 vertebra is hanging over the L5. The neurosurgeon says spine surgery with nuts, bolts & plates is needed. I have rejected the surgical option for now.
What is the long-term outcome if nothing is done? Will I be a handle pain for now
Just how will it affect me other than pain over the long term?
I can handle the pain for now; please advise. How will it affect me other than pain over the long term?
Dear Trish,
Please forgive us for not replying sooner. From your description, it appears that you have a spondylolisthesis. Spondylolisthesis is a congenital or developmental disorder of the spine that leads to a forward displacement of a spinal bone. In general, there are two types; stable and unstable.
Unstable spondylolisthesis is prone to progression and can rapidly progress through the four stages. Condition is graded based on severity, ranging from grade 1 to 4. A grade-1 describes an instance where the forward slippage ranges from 0 to 24%. A 25-49% slippage is classified as a grade-2. Grade 3 is 50-74%, and grade 4 is an instance where the slippage is more than 75%.
Here are some helpful links:
https://www.mychiro.com.my/articles/spondylolisthesis/
https://www.mychiro.com.my/conditions/sciatica-spondylolisthesis/
https://www.chiropractic-in-malaysia.com/blog/spondylolisthesis-spondylolysis-treatment-kl
Developmental forms of spondylolisthesis are entirely due to degenerative changes or premature wear and tear. In all cases, spondylolisthesis presents with slipped discs (bulging or herniated discs), hypertrophy of facets (degenerative arthritis of spinal joints), and hypertrophy of ligamentum flavum. The combined effects cause shrinkage of the spinal canal and impingement of nerves.
The main issue with spondylolisthesis is that it is a progressive condition. You don’t have to have surgery to stabilize it or to get rid of the pain. You must treat it as early as possible to avoid severe pain or disability.
How bad can it get?
Spondylolisthesis can become quite unbearable and may lead to disability, including paralysis.
Are there any alternatives to surgery for spondylolisthesis?
If you have spondylolisthesis, a conservative course of action is your first step. However, conservative care or treatment must be precise and personalized to each patient with spondylolisthesis.
What types of treatment or activities should to avoid?
You should avoid any bending or twisting movements. Do not do Yoga or Mckenzie exertion exercises.
Can chiropractic help patients with spondylolisthesis?
Chiropractic is excellent for patients with spondylolisthesis. However, it must be through either the Activator methods or Thompson.s. Try to combine your chiropractic treatment with physiotherapy (physical therapy) during the same session for the best results.
Here is a helpful link on chiropractic treatment techniques:
https://www.mychiro.com.my/articles/gonstead-diversified-and-activator/
https://www.yourchiro.com.my/blog/chiropractic-technique/
Avoid the rotatory methods of chiropractic, including the Diversified and Gonstead methods. I hope this helps, do contact us on 03 2093 1000 or Whatsapp us at +(60)17 269 1873 for more information.
What do you recommend? What should one do if surgical fusion fails? For example, what to do for persistent pain after spine surgery that fussed the L4 and L5 with bars, plates, and screws?
Dear Tammie,
We apologize for not getting back to you soon enough. Spine surgery is not a cure. Spinal fusion is an aggressive surgical intervention using screws, rods, and plates to fuse segments. Contrary to common belief, fusion surgeries at L4-L5 will not cure the pain or condition. According to published research that reviewed the success rate of spine fusion in over 1,400 patients, 74% of patients will have residual pain.
Once the spine is fussed, there is no further surgical intervention. However, that doesn’t mean that there is nothing that you can do! To eliminate the pain, you need precision treatments by our chiropractors and physiotherapists. Post-surgical pain, especially those resulting from fusion, needs specialized skill sets and advanced therapy devices. Patients with failed spine surgery or post-surgical pain must avoid any therapy or exercise that twists or bends the spine. Yoga, twisting, or turning at the waist is destructive and harmful.
If you live in Malaysia or if you can visit our Chiropractic Specialty Center® in Kuala Lumpur, we can help.
I am 51 years. After recovering from covid, I had severe pain in my back while walking and standing. I was advised to rest. My MRI report says I have L4-L5 listesis (spondylolisthesis). I am on medication and light exercises. Pain persists. Please advice.
Dear Arindam,
Listheisis means slippage, which is commonly caused by spondylolisthesis. Spondylolisthesis is a spinal condition where one vertebra slips forward or backward relative to the adjacent vertebrae. This can lead to compression of the nerves and spinal cord, resulting in back pain, muscle weakness, and numbness or tingling in the legs. Various factors, including degenerative changes, trauma, or genetic predisposition, can cause spondylolisthesis. The best treatment option for spondylolisthesis is NSD Therapy® combined with spondylolisthesis-specific methods of chiropractic and physiotherapy.
Unfortunately, there is little I can tell you online that would make a difference. I need to assess you and review your MRIs in detail before I can help. Please WhatsApp my office if you wish for me to assess you
My MRI shows my intervertebral disc heights at:
• L1-at 11 mm
• L2-at 9.4mm
• L3- at 1mm
• L4-at 7.4mm
• L5-at 9.9 mm
I can walk up to one minute. I have been suffering from this problem for the last 2 months. Please suggest what I should do now. I am residing in India.
Thank you for reaching out and sharing the details from your MRI. Based on the measurements you’ve provided, it appears you are experiencing significant spinal challenges, particularly with the very narrow disc space at L3, which measures only 1mm. This condition indicates severe spinal canal stenosis, which can lead to serious complications such as difficulty walking, foot drop, and potentially even cauda equina syndrome.
Given the severity of your condition, especially if the measurement at L3 is accurate, surgical intervention might be necessary to prevent further deterioration and alleviate the symptoms. However, there are conservative treatment options that could also be considered, particularly if you are looking for non-surgical alternatives.
At our center in Kuala Lumpur, we specialize in a comprehensive approach to spine care that includes advanced non-surgical treatments. These treatments are not commonly available in India, where the practice of chiropractic care might differ significantly. It’s important to note that in India, individuals offering chiropractic services might not be formally trained or certified as chiropractors from an accredited chiropractic university, which is essential for ensuring safe and effective care.
Our treatments include:
• Non-Surgical Spinal Decompression: Utilizes a decompression table to gently stretch the spine, which can help alleviate pressure on the compressed nerves.
• Physiotherapy: Customized exercises and modalities to strengthen spinal support and increase mobility.
• Chiropractic Adjustments: Performed by certified chiropractors who are trained to safely adjust the spine and improve alignment.
If you plan to visit Kuala Lumpur, I would be more than happy to assess your condition in person and discuss how we can help manage your symptoms conservatively. If you’re seeking chiropractic care in India, please ensure that the practitioner has a legitimate degree in chiropractic from a recognized institution.
For further information or to schedule an appointment at our Kuala Lumpur center, please feel free to contact us. Your health is of utmost importance, and we are here to provide the highest standard of care.
Dear Dr Yama Zafer,
I am 65 years old and have just finished reading your detailed post on L4 L5 S1 disc herniation. Thanks for the beautiful elaboration. I have had mild to, at times, severe lower back pain on the left that runs into the left hip joint. My pain started about 6-7 months ago and I have a bit of side leaning to the right while walking.
However, for the last month, I have been having severe pain in the left hip joint radiating down to the left foot. Now standing and walking causes unbearable pain. A Recent MRI showed:
• L4-S1: An L4-L5 disc bulge with posterior-central disc extrusion and inferior migration causes severe spinal canal and bilateral neural foraminal stenosis (severe). The migrated components measure 6.5mm and impinge on the bilateral traversing nerve roots more on the left.
• L5-S1: A mild disc bulge causes mild spinal canal and bilateral moderate neural foraminal stenosis without impingement of nerve roots.
I would be highly thankful if you could kindly suggest a remedy.
Regards,
Brijesh Kumar
Dear Brijesh Kumar,
Thank you for reaching out and for your kind words about the L4 L5 S1 disc herniation post. Your detailed description of your symptoms and MRI results helps greatly in understanding the severity of your condition.
The MRI findings indicate significant issues at the L4-L5 level with a disc bulge and posterior-central disc extrusion that has migrated, causing severe spinal canal and bilateral neural foraminal stenosis. This condition is indeed serious, especially given the impingement on the bilateral traversing nerve roots, more so on the left, which correlates with the severe pain you are experiencing radiating from the hip to the foot.
At our center, we specialize in non-surgical treatments that are specifically designed to address severe spinal conditions like yours without exacerbating the issue. Here’s what we can offer:
• Chiropractic Care: Our chiropractic treatments are disc-specific and avoid general manipulations that could stress the disc further, such as Diversified and Gonstead methods that involve side-posture treatments. Instead, we use techniques that safely manage disc herniations without twisting or rotating the spine.
• Spinal Decompression Therapy: This non-invasive therapy gently stretches the spine, which can help relieve pressure on the affected discs and nerve
• High-Intensity Laser Therapy: This therapy helps reduce inflammation and pain at a cellular level, promoting faster healing.
• Manual Soft Tissue Manipulation: Focused on improving mobility and alleviating tension in the muscles and connective tissues surrounding the affected area.
• Physiotherapy: Tailored exercises and treatments that strengthen the supporting musculature and improve overall spinal health, carefully designed to avoid any positions that may worsen the condition, such as the cobra pose or McKenzie exercises.
Given the complexity of your condition, a personalized, comprehensive approach is essential. I strongly recommend scheduling a consultation at our center where we can assess your specific needs and develop a detailed treatment plan. We have had considerable success treating similar and even more severe conditions, and we are confident we can help alleviate your symptoms and improve your quality of life.
Please contact us via WhatsApp at +6017-269-1873 to schedule an appointment or to discuss your condition further. We are here to provide the care you need and ensure a thorough understanding of all available treatment options.Looking forward to the opportunity to assist you on your path to recovery.
Warm regards
I’m 26 years old, and I’m suffering from disc bulge lumber and cervical spine. What can be done, and is this a condition you can help with?
Dear Adil,
Thank you for reaching out about your concerns with disc bulges in both your lumbar and cervical spine. At your age, addressing these issues proactively is crucial to manage symptoms and prevent further progression.
Disc bulges can lead to discomfort and limitations, but many individuals experience significant improvement with the right approach. At our center, we specialize in non-surgical care designed to target the root causes, repair damaged tissue, and alleviate the pain and other symptoms associated with disc bulges. Our approach includes:
You will need focused chiropractic and physiotherapy combined with rehabilitation, interactively targeting the damaged spinal discs. The chiropractic and physiotherapy care you receive must be highly peroslazied and non-rotatory. In other words, you should never have your back twisted, roasted, popped, or cracked if you have a slipped disc (bulging or herniated discs). In chiropractic and physiotherapy, there are alternative deviance-based methods, precisely for patients with disc issues, and we are highly efficient in them.
These treatments, combined with lifestyle modifications and regular follow-ups, have helped many of our patients lead a more comfortable life. Each treatment plan is customized based on individual assessments, ensuring that you receive the most effective care suited to your specific needs.
If you are interested in learning more about how we can help you, or if you wish to schedule an appointment, please WhatsApp us at +(60)17-269-1873. We are here to assist you in managing your condition and improving your overall spine health.
Best regards,
Hello,
I have shooting pain on both sides down to my feet. MRI was done and now I need help. Could you please provide an interpretation of the following MRI report? Is it indicative of a good or bad condition? Additionally, what steps should I take if the MRI report indicates a problematic condition?
General MRI Findings:
T10-11: Mild disc bulge. Non-compressive posterolateral ligamenta flava thickening.
T11-12: Mild disc bulge. Normal cord and spinal canal.
T12-L1: Mild disc bulge. Normal conus and spinal canal.
L1-2: Diffuse disc bulge. Normal spinal canal.
L2-3: Diffuse disc bulge. Mild neuroforaminal narrowing. Patent L2 exiting roots and DRG. Capacious central canal and lateral recesses.
L3-4: Diffuse disc bulge. Mild neuroforaminal narrowing. Patent L3 exiting roots and DRG. Capacious central canal and lateral recesses.
L4-5: Diffuse protrusion. Severe neuroforaminal narrowing. L4 exiting roots and DRG are impinged bilaterally.
L5-S1: Diffuse protrusion. Severe neuroforaminal narrowing. L5 exiting roots and DRG are impinged bilaterally.
Regards,
Fadzlee
Hello Fadzlee,
Thank you for reaching out and sharing the details of your MRI report. Based on the findings you’ve provided, it appears that you are experiencing significant spinal issues that are contributing to the shooting pain down both sides to your feet. Here’s a detailed interpretation of your MRI findings and recommendations for next steps.
MRI Report Interpretation:
Your MRI shows several levels of disc bulging from T10-L1, which are mild and do not seem to be compressing the spinal cord or nerve roots significantly. These mild bulges might not be the primary cause of your severe symptoms but could contribute to discomfort.
At the levels L4-5 and L5-S1, there are more concerning findings:
Diffuse Protrusions with Severe Neuroforaminal Narrowing: This condition is where the nerve passages at the sides of the vertebrae (foramina) are severely narrowed due to bulging discs. This narrowing is impinging, or compressing, the nerve roots (L4 and L5 exiting roots and DRG – Dorsal Root Ganglia) on both sides. This impingement is likely the primary cause of the shooting pain you are experiencing in your legs.
Evaluating the Condition:
• Severity: The conditions at L4-L5 and L5-S1 can be considered serious due to the bilateral impingement of nerves. This typically results in significant pain, numbness, or weakness extending down the legs, which matches the symptoms you describe.
• Good or Bad: The overall condition could be deemed problematic due to the presence of nerve impingements, which require careful management to prevent further damage and alleviate symptoms.
Recommended Steps:
• Consultation with one of our chiropractors in Kuala Lumpur: It’s crucial to have a consultation and follow-up with one of our chiropractors as we provide non-surgical options. Spine specialists, such as orthopaedic and neurosurgeons, may recommend surgery. However, based on what you have mentioned, your condition will most likely respond favourably to our methods of spinal disc rehabilitation through chiropractic, physiotherapy, and rehabilitation. Over the last three decades, I have treated thousands of patients with L4-L5 and L5-S1 issues, the majority of whom never recovered fully without the need for spine surgery. I encourage our methods as it is the most comprehensive spine care given by chiropractors and physiotherapists during the same session.
• Consideration of Surgery: If conservative treatments do not alleviate the symptoms and the nerve impingement is severe, surgical options like a decompression surgery or a discectomy might be considered to relieve the pressure on the nerves.
• Lifestyle Adjustments: Modify activities that exacerbate the pain and consider ergonomic adjustments to reduce strain on your spine during daily activities.
Long-Term Management:
Managing a condition with severe neuroforaminal narrowing requires a comprehensive approach. I recommend our integrative rehabilitative approach over what others may recommend. If you follow our recommendation, long-term management should be favourable as well.
If you would like to schedule an appointment with me or one of our other chiropractors, please WhatsApp our main center at +(6017-269-1873; I hope this helps.
Last 30 days I have been suffering from Lower back pain.
Here are the impressions of my lumbar MRI:
• Straightening of lumbar spine noted.
• Anterior marginal osteophytes at all levels.
• Disc desiccation was noted at L4-L5 levels.
• L4-L5: Large postero-central disc protrusion causing marked compression in the central canal
• and left lateral recess.
• Visualized vertebrae are normal in height, alignment, MR morphology, outline and signal
• intensity.
• The yellow ligament is normal in thickness.
• Facet joints are normally visualized.
• Conus medullaris is normal in position and signal intensity pattern.
• Visualized soft tissues are normal in signal intensity.
• Bilateral sacroiliac joints show normal hyperintense signals, suggesting maintained joint
• spaces.
• The spinal Canal diameter is as follows:
• L1/2-10.5 mm, L2/3- 9.5 mm, L3/4-8.0 mm, L4/5-3 .5 mm and at L5/S1-11.0 mm.
Kindly guide my present condition
I am 43 years old with back pain. It all start during off-road traveling 30 days ago. Could this be due to a slipped disc and if so what can be done?
Dear Gangadhara,
Firstly, we sincerely apologize for the delay in responding to your query posted in December. We strive to provide timely and helpful replies, but unfortunately, we missed your important question. We appreciate your patience and value your interaction with our blog.
Based on your MRI findings, it appears you have several challenges in your lower back, particularly the large postero-central disc protrusion at the L4-L5 level, which is causing significant compression in the central canal and affecting the left lateral recess. This compression can contribute to your lower back pain and may also impact nerve function.
Key MRI Impressions:
• Straightening of the lumbar spine and anterior marginal osteophytes suggest some degree of spinal degeneration and stiffness.
• Disc desiccation at L4-L5 indicates that the disc has lost hydration, which can reduce its ability to cushion the vertebrae.
• The narrowing of the spinal canal at L4-L5 (3.5 mm) is particularly concerning as it signifies severe spinal stenosis at this level, which can compress the spinal cord and nerves.
Managing conditions like yours involves a comprehensive and conservative approach, especially since certain movements and therapies could exacerbate your condition. It is crucial to avoid bending, twisting, or any extension exercises such as the cobra pose or McKenzie back exercises. These activities could further reduce the size of the spinal canal, increasing compression and pain.
What We Offer at CSC:
At Chiropractic Specialty Center®, we provide a blend of integrative methods combining the expertise of chiropractors and physiotherapists. Our approach includes:
• Decompression Therapy: To gently stretch the spine and relieve pressure.
• Ultrasound Therapy: To promote tissue healing.
• Spinercise Rehabilitation: To strengthen the spine safely.
• Flexion-Distraction Therapy: To increase spinal motion without stress.
• Laser Therapy: For pain relief and inflammation reduction.
• Manual Physiotherapy Procedures: For targeted physical rehabilitation.
• Non-rotatory Chiropractic Treatments: Using safe techniques like the SOT, Activator Methods, or Thompson Technique, avoiding any rotational spinal manipulations that could harm your condition.
Personalization of therapy is key to effectively managing and potentially improving your condition without the need for invasive procedures.
I strongly recommend booking an appointment for a thorough assessment at our center. We can then discuss in detail how our targeted, evidence-based conservative care can address your specific needs and help manage your symptoms. Please contact us via WhatsApp at +6017-269-1873 to schedule your visit. Looking forward to helping you regain comfort and improve your spinal health.
Hi,
What does this mean? L4-L5 is the seat of a right lateral protrusion.
Hello,
Thank you for reaching out with your question about your diagnosis. The phrase “L4-L5 is the seat of a right lateral protrusion” refers to a condition in your lower back, specifically between the fourth and fifth lumbar vertebrae. Here, “lateral protrusion” indicates that the disc material is bulging out towards the right side of your spine.
This bulging can pressure or irritate the nearby nerves, potentially causing pain, numbness, or weakness in the lower back, hip, or leg on the right side. It’s important to address this condition to prevent further discomfort or more severe issues.
If you’re experiencing any related symptoms or would like a more detailed explanation and personalized advice on managing this condition, please do not hesitate to reach out. You can contact us via WhatsApp at +6017-269-1873 for a consultation or more information on our chiropractic, physiotherapy, and rehabilitation options.
Hi!
I am 20 years old. And I am suffering from an L4-L5 disc bulge. It was diagnosed last August -September period. I underwent physiotherapy. It’s fine. But sometimes the pain triggers again and causes my left leg to pain harder. What should I do? The doctor prefers surgery, which I don’t want to.
Dear Vaishnavi,
Thank you for reaching out and sharing your concerns about your L4-L5 disc issue. I understand your hesitation regarding surgery, especially at your young age of 20. It’s important to explore all non-surgical options that can provide lasting relief and address the root cause of your pain.
At CSC, we specialize in managing conditions like yours through a combination of chiropractic care, focused physiotherapy, and comprehensive rehabilitation. These plans are designed to not only alleviate pain but also to strengthen your spine and prevent future episodes. Given that the pain sometimes triggers and affects your leg, it suggests that the disc issue may be impacting nearby nerves.
A bulging disc, often referred to in medical terms as a protrusion, prolapse, herniation, extrusion, or fragmentation, describes various stages where the disc material extends beyond its usual boundaries. This can occur without symptoms, but pain arises when the disc material begins to press on spinal nerves. Your description suggests that the disc may not just be bulging but could be herniating, which requires targeted intervention to prevent worsening.
We strongly believe that surgery should be a last resort, especially for someone as young as you are. Our experienced team of chiropractors and physiotherapists can provide a thorough assessment and work with you to create a personalized plan focused on non-invasive recovery methods.
I invite you to visit our center for a consultation where we can discuss your condition in more detail and explore the best treatment options. Please contact us at +6017-269-1873 to schedule your appointment. We’re here to help you understand your condition better and guide you towards lasting relief.
Can you call me for a appointment
Certainly! Please contact us on our main office’s WhatsApp line at +6016-269-1870 to schedule your appointment. We look forward to hearing from you and are here to assist you at your convenience. Thank you!
My L4 and L5 vertebrae are rubbing on the nerves. My spinal disc has degeneration and bulging. I’m in physical therapy for the discs for my current condition which may have resulted from a previous injury where my pelvis was crushed in a car accident. I’m in a lot of pain, feeling pain in my back. Leg and toes. I’m m also trying to lose weight to take pressure off the nerves in my lower back. Are there any other therapies or procedures that I can do to slow down my deterioration?
Dear Natalie,
Managing pain from conditions like spinal disc degeneration and nerve compression can be challenging, but it sounds like you’re already taking positive steps with physical therapy and weight management. Here are some additional therapies and strategies, including a specific chiropractic method that might help slow down deterioration and alleviate your symptoms:
Spinal Decompression Therapy: This non-surgical treatment uses a traction table or similar device to gently stretch the spine, relieving pressure on the discs and nerves, which can reduce pain and promote healing of damaged discs.
Aquatic Therapy: Also known as hydrotherapy, this involves using the resistance and buoyancy of water to help relieve pain, improve mobility, and strengthen muscles without putting stress on the spine.
Acupuncture: Some find relief through acupuncture, which involves inserting thin needles into specific points on the body to stimulate the nervous system and enhance natural painkillers.
Anti-Inflammatory Diet: Consuming foods that reduce inflammation, such as those rich in omega-3 fatty acids and various fruits and vegetables, might help alleviate some pain.
Chiropractic Care – Activator Method: This gentle, non-invasive technique uses a hand-held device to deliver precise, controlled thrusts to specific areas, without the need for twisting or forceful manipulation. It’s especially suitable if you have concerns about exacerbating disc and joint issues. This method minimizes discomfort and maximizes the effectiveness of the adjustment, making it a safe option for those with delicate conditions.
Regular Exercise and Stretching: Gentle exercises that strengthen the core and lower back can support spinal health and reduce nerve pressure.
Pain Management Clinics: These offer comprehensive approaches to pain management, including physical therapy and more targeted interventions, depending on the severity of your condition.
Discuss any new therapies with your healthcare provider to ensure they’re suitable for your health needs, and consider consulting with a specialist trained in the Activator Method for targeted, safe chiropractic care.
Hi my mother aged 62 generally complains for excessive leg pain (especially calf muscles ). MRI Lumbar spine Scan has given following impression (1) Mild Lumbar Spondylolysis (2) Minimal Scoliosis of spine towards right side(3) L3 l4 disc minimal bulge indenting thecal sac and bilateral traversing nerve roots (4) L4-5 disc moderate diffuse bulge compressing thecal sac stenosing bilateral leteral recesses& neural foraminae with impingement of bilateral traversing nerve roots.
Neuro surgeon advises for surgery to relieve nerves , can you please suggest any non surgical options and chances of success of non surgical options . patient is based in Bangalore . Any right doctor or practitioner of non surgical therapies in Bangalore is highly desirable
Dear Ranjit,
It sounds like your mother is dealing with several spine-related issues, which can indeed be quite painful and impact quality of life. At CSC, we specialize in non-surgical options that could potentially help manage and alleviate her symptoms. Here’s an overview of what we offer and how these might benefit her:
Non-Rotatory Chiropractic Care: This type of chiropractic care avoids twisting the spine, which is particularly important given your mother’s conditions like scoliosis and disc issues. It focuses on gentle techniques that align the spine and relieve pressure on the nerves.
Physiotherapy: This includes a range of therapies through machines and hands-on care including exercises, stretching, and strength training designed to improve mobility, strengthen the muscles supporting the spine, and decrease pain. For your mother, specific exercises can be tailored not to exacerbate her scoliosis and spondylolysis.
Spinal Decompression Therapy: This therapy uses a traction table or similar motorized device to stretch the spine. This can help relieve back and leg symptoms by taking pressure off compressed discs and nerves (like those affecting your mother at the L3-L4 and L4-L5 levels).
Rehabilitation: Comprehensive rehabilitation programs aim to improve overall strength and function, which can help stabilize her spine and reduce the symptoms of spondylolysis and the effects of scoliosis. Rehabilitation can also aid in recovery from or prevention of further deterioration due to her disc issues.
The success of Non-Surgical Options
The success of non-surgical care varies based on individual conditions, the severity of the issues, the therapy center, and how the patient’s body responds to treatment. Many patients find significant relief from combinations of these therapies, especially if surgeries are considered high-risk or if patients prefer less invasive approaches. It’s also important to start these treatments under the guidance of skilled practitioners who can adjust therapies as needed.
Finding the Right Practitioner in Bangalore
Although I don’t have access to browse specific practitioners in Bangalore, I would recommend seeking out a reputable clinic that offers a multidisciplinary approach. Look for centers that specialize in non-surgical spine care and have a team that includes chiropractors, physiotherapists, and possibly specialists in spinal decompression. Checking patient reviews and asking for referrals from her current healthcare providers or local medical associations can also help in choosing the right clinic.
Addressing the root causes of her symptoms through these non-surgical therapies has a good chance of improving her condition and reducing the need for surgical intervention. It’s important to have a thorough assessment by non-surgical specialists who can develop a personalized treatment plan tailored to her specific needs.
I just found out my boyfriend has L4-L5; there is no spinal canal stenosis or narrowing and there is a Small bulging disc at L5-S1; I would love to be informed more by anyone who can give me some details on the do’s and don’t he will need to help him prevent worsening. Much appreciated!!
Dear Sabrina,
It’s great that you’re seeking information to support your boyfriend! Here’s a simplified explanation of his condition and some general advice on managing it:
L4-L5; No Spinal Canal Stenosis or Narrowing: This indicates that at the segment between the fourth and fifth lumbar vertebrae, there is no significant narrowing of the central canal where the spinal cord travels. This is good news because it means there’s less risk of nerve compression in that particular area, which can cause pain or mobility issues.
Small Bulging Disc at L5-S1: This refers to a slight disc protrusion between the fifth lumbar vertebra and the first sacral segment. While labeled as small, it can still cause discomfort or pain if it presses on nearby nerves.
Do’s and Don’ts for Managing the Condition:
Do:
Maintain good posture: Keeping the spine properly aligned can help prevent additional stress on the affected discs.
Stay active: Regular exercise, especially activities that strengthen the core and back muscles, can support the spine. Swimming, walking, and yoga are often recommended.
Use proper lifting techniques: Bend at the knees and keep the back straight when lifting objects to avoid strain.
Stay hydrated: Drinking plenty of water helps keep the discs hydrated and healthy.
Don’t:
Engage in high-impact activities: Sports or exercises that involve jarring or heavy impacts can aggravate the condition.
Lift heavy objects improperly: This can put more pressure on the discs and spine.
Sit for prolonged periods: Frequent breaks to stretch and move around are important if he has a sedentary job or lifestyle.
Ignore pain: If he experiences increased discomfort or new symptoms, consulting a healthcare provider is crucial.
Overall, maintaining a healthy lifestyle with regular exercise and good ergonomics can greatly help manage and prevent the worsening of a bulging disc.
It might also be helpful to consult with a chiropractor, your doctor, or a PT who can provide personalized guidance and therapy plans.
What does L4-L5 failure of a right lateroforaminal herniation mean? what does C5-C6 is the site of a median protrusion mean?
What does L4-L5 is the site of a right lateral herniation mean?
Dear Carla,
Here’s a straightforward explanation for the terms mentioned in the question:
L4-L5 Failure of a Right Lateroforaminal Herniation: This term refers to a specific type of herniation at the lower back, between the fourth and fifth lumbar vertebrae. “Lateroforaminal” means the herniation is happening toward the side and near the opening where nerves exit the spine, which can cause pain or discomfort typically on one side of the body. “Failure” here might refer to the herniation not responding to treatments or getting worse, but it’s a bit unusual to see “failure” used in this context without additional explanation.
C5-C6 is the Site of a Median Protrusion: This refers to a herniation in the neck area, specifically between the fifth and sixth cervical vertebrae. “Median” means the herniation is centrally located and might be pushing directly towards the spinal canal, which can affect the spinal cord and potentially cause symptoms like pain, numbness, or weakness in the arms or shoulders.
L4-L5 is the Site of a Right Lateral Herniation: Similar to the first explanation but clarified here, this is about a herniation also at the lower back, but “lateral” means explicitly it is protruding toward the side. This can impact the nerves on that side, possibly causing pain or numbness in the leg or hip on the right side.
Understanding these terms can help you discuss treatment options more effectively with your healthcare providers. If you have these conditions, it’s essential to consult with a specialist who can offer tailored advice and care plans. I hope this helps.