Thinking about spine surgery or trying to avoid it? This page explains what common procedures (laminectomy, discectomy, fusion and “minimally invasive” versions) aim to do, the risks they carry, and why published “success” in studies can differ from what patients call success in real life.
You’ll see when surgery is usually considered, who shouldn’t delay urgent assessment, and what a measured, non-invasive plan looks like (calm-first, image-informed, non-rotatory, with clear checkpoints). We also walk through research on real-world outcomes, discuss options like NSD Therapy® (a gentle, customizable protocol), and give practical questions to ask before choosing your path. The goal: help you make a safer, clearer decision with your registered clinician based on your goals, not headlines.
Key takeaways
“Successful” in studies isn’t the same as success for you. Ask how your result will be measured pain, function, sleep, meds, work. You deserve clarity.
Surgery is for clear red flags or proven compression that didn’t improve with good care. Many others can start safely with non-invasive options.
Good conservative care is calm-first and precise. No forceful twisting in flares, image-informed decisions, dose-controlled modalities, and regular checkpoints.
Set patient-meaningful goals and track them. Pain ≤3/10, walk/sit 30–60 minutes, fewer meds, better sleep, back to roles. Review at weeks 2/4/8 and adjust.
If one surgery didn’t help, pause. Re-diagnose, try a time-boxed gentle plan, and get both surgical and non-surgical opinions. NSD Therapy® is a tailored, low-force option for selected cases.
Educational information only. Make decisions after a thorough exam with a registered clinician.
What “successful” means in research vs what it means to you
In clinical papers, “success” often means any measurable improvement for example, a small drop in a pain score or a modest gain on a disability index. By that definition, moving from pain 10/10 to 9/10 can be counted as a success.
For most patients, success means something different: pain low enough to live normally, fewer meds, better sleep and walking tolerance, and a return to work or sport. That gap in definitions is why some procedures are reported as “successful” in journals while many people still report persistent symptoms afterward.
The Merriam-Webster Dictionary defines success as a “degree or measure of succeeding.“ In other words, any improvements or gains are considered successes. A spine surgeon may view the surgical intervention as successful when patient symptoms decrease or when the quality of life increases.
Large observational cohorts have also shown mixed real-world results for certain surgeries (e.g., lumbar fusion showing low return-to-work rates and higher reoperation/complication and opioid-use rates in specific populations). These data don’t apply to everyone, but they’re a reminder to look beyond headlines and understand how “success” was measured (Nguyen et al., Spine 2011).
It’s crucial for patients to explore all available options and consult with healthcare professionals to determine the most appropriate course of action for their specific condition.
When surgery is usually considered
Surgery tends to be reserved for situations such as:
Clear structural compression with correlating symptoms that do not respond to a well-run, time-bound course of conservative care
Instability, deformity, fracture, infection, or tumor where operative care is standard
Outside of these, many people improve with a measured, non-invasive plan.
What non-invasive care can offer
A good conservative program is targeted, gentle, and staged:
Starts with calm-first strategies (no forceful twisting or end-range “cracking” during inflammatory phases)
Uses image-informed decision-making when available (correlate exam with MRI findings)
Applies dose-controlled modalities (e.g., angle-controlled decompression, flexion–distraction, high-intensity laser, therapeutic ultrasound, focused shockwave at low settings when indicated)
Adds movement re-education and core control only when tissues tolerate loading without flare-ups
Reviews progress at set checkpoints and adjusts the plan
A practical way to judge “success” (patient-centered, not just study-centered)
Before choosing surgery or a non-invasive plan, agree with your clinician on clear, patient-meaningful targets, such as:
Pain ≤3/10 most days
Walking/sitting tolerance (e.g., 30–60 minutes without a spike)
Medication reduction (e.g., step-down of opioids/NSAIDs if you’re using them)
Function (return to work/household roles/sport tasks)
No new neurological deficits
Ask how and when these will be measured (e.g., at 2, 4, and 8 weeks) and what the next step is if targets aren’t met.
Questions to ask whichever path you take
How is “success” defined for me, not just in studies?
What are the likely risks/complications in my situation?
What non-surgical options are left to try, and for how long, with what checkpoints?
If I improve only a little, what’s Plan B? If I worsen, what’s Plan C?
How will we track progress (pain, function, meds, return-to-work)?
Educational information only; not medical advice. Decisions should follow a thorough assessment by a registered clinician. Individual results vary.
Key Considerations Before Opting for Spine Surgery
When contemplating spine surgery, patients should weigh several critical factors:
Risk of Complications:Surgical procedures can lead to complications such as infections, nerve injuries, and hardware failures. Understanding these risks is essential.
Success Rates:Success is subjective; while a procedure might be deemed successful clinically, patients may continue to experience symptoms post-surgery.
Non-Invasive Alternatives:Before deciding on surgery, exploring non-invasive care like chiropractic care, physiotherapy, and rehabilitation can be beneficial. These methods have shown efficacy in managing spinal conditions without surgical intervention.
Informed decisions, guided by thorough consultations with healthcare providers, can lead to better outcomes and patient satisfaction.
Consult Our Experts for Personalized Spine Care
If you’re considering spine surgery or seeking alternatives, our team at Chiropractic Specialty Center® is here to assist.With a focus on non-invasive care, we offer comprehensive evaluations and personalized care plans tailored to your needs.Our integrative approach combines chiropractic, physiotherapy, and rehabilitation therapies to address spinal conditions efficiently.
Don’t make decisions about your spine health without exploring all options.Reach out to us today to schedule a consultation and discover how our non-surgical methods can benefit you. Contact Us
Conservative Care Of The Spine Offers Better Results Than Surgery.
If you experience back or neck discomfort, you might reconsider having spine surgery. The general rule is to get focused on conservative care before thinking about spine surgery. The therapeutic technologies and devices available today have dramatically improved the non-surgical methods of spine care. The most efficient of these methods is NSD Therapy®. NSD Therapy® is an integrative method of care given by chiropractic and physiotherapists combined. The NSD Therapy® system incorporates integrated therapy devices such as the RxDecom, Shockwave therapy, high-intensity laser therapy, and several other therapeutic devices, depending on the need.
In the coming sections, we will describe spine surgery in detail. We have also provided an example of a patient we care for who was told that surgery was successful. It may have been successful from a clinical standpoint, but he was still unable to live an active life. We have discussed the case below:
Real-Life Case Of A Reported Successful Back Surgery?
A case that comes to mind is a male patient who presented to our center with severe, excruciating discomfort in his lower back and legs.
In addition to discomfort, he suffered from significant weakness in his legs, resulting in a foot drop. The severity of discomfort prevented the patient from sleeping or participating in any physical activity. After consulting his surgeon and us, the patient chose the surgical route with the surgeon-recommended laminectomy or fusion (minimally invasive spine surgery).
Immediately after the surgery, his lower back and legs’ discomfort decreased by more than 50%. His spine surgeon considered the minimally invasive spine surgery as successful, and within days the patient was scheduled for post-surgery rehabilitation. Physical therapy and home care exercises were provided to the patient, and the patient was discharged from the hospital.
Post-surgical care and home care exercises provided minimal improvements. However, the prolonged sitting, standing, and even walking were still uncomfortable. The patient continued to walk with a noticeable limp and complained of moderate back discomfort, leg discomfort, and pins and needles in his legs, feet, and toes. Clinically you could argue that this was a successful spine surgery, and you would be right to a certain extent. However, from a patient’s perspective, the outcomes were not as favorable as they should have been.
Six Months Later
Six months after his spine operation, he still suffered from a mild foot drop, weakness in the legs, inability to walk more than 200 meters, and inability to sit for prolonged periods.
In short, he was unable to continue with the life he knew. This is the story of just one patient. But many have similar faith when they opt for surgical interventions without exhausting efficient conservative means of non-invasive therapy.
Back discomfort sufferers are often told that spine surgery is successful in 90% of cases. What most neglects to elaborate on is the degree of success in both the short and long term. While it is true that surgery can reduce the level of annoyance and discomfort, sufferers often continue to have residual discomfort of varying degrees.
Published research articles often portray spine surgery success rates from 50%-90%, depending on the source you come across. The differences in rates of improvement depend on the severity of the condition and, of course, on the researcher’s established protocols and guidelines that define postoperative clinical successes. Therefore, it is not your surgeon who provided the wrong information. The surgeon is just relaying the published literature.
Although strict publishing criteria exist, the vetting of research material is a daunting task for publishers to assess the provided research article thoroughly. Furthermore, most surgeons publish successful patient cases. Rarely will a surgeon release for publication a failed surgical intervention.
Also, a researcher who obtained research grants from implant manufacturers may have an affinity towards publishing articles favorable to implants. Although there are strict criteria for disclosing conflicting interests, some may have discovered means that avoid it. In short, published research is not flawless in claims of success.
Why Is Conflict Of Interest In Medical Research So Rampant?
The National Academies Press in Washington, D.C. (United States of America) published the results of surveys approved by the U.S. Governing Board of the National Research Council that showed the extensiveness and assortments of dealings and associations between physicians and industry researchers, and academic educators in reputable universities. They reported such conduct was universal in academia, teaching hospitals, and societies (associations).
Researchers getting gifts from drug companies is extremely rampant;
Drug companies and medical device companies continual visiting of doctors’ offices with free samples is widespread;
The vast majority of biomedical research in the United States is made possible by grants and financial help from the industry (pharmaceuticals and medical device manufacturers);
Academic researchers in Universities or teaching hospitals put their names on pre-written research paid for the publication by pharmaceutical companies, medical device manufacturers, surgical implant makers, and other industry players;
Professional societies (medical associations or other groups) provide research materials without disclosing the source of their funding or conflicts of interests of the authors who drafted the research article.
Insights Into Why There Are So Many Conflicting Reports About The Clinical Successes Claimed By Most Regarding Spine Operations.
We found a few articles when we set out on a mission to find surgical complications related to spine surgery. The vast majority of articles published were favorable of spine surgery in the short and long term. Therefore, we changed our search criteria and started to look at published research on governmental agencies’ compiled data. We were astonished by what we discovered in published research from the Ohio Bureau of Workers’ Compensation database. Before discussing the merits or importance of this published research, let’s go over the common types of spine surgery.
Different Types Of Back Operations Procedures
In general terms, spine surgery is performed when the spinal nerve, spinal cord, or thecal sac (housing of the spinal cord) are compressed to the degree that causes significant symptoms. Three main disorders that lead to such compression are:
The primary goal of spine surgery is to decompress damaged tissue’s compressive effects, either by cutting or instrumentation (plates, rods, and screws). In some cases, both cutting and instrumentation are used. Decompression spine surgery involves the removal of structures or tissues that are compressing and putting pressure on nerves. There are several methods, and we shall discuss them briefly below.
Spinal decompression surgeries are sometimes touted as minimally invasive spine surgery. They are called minimally invasive spine surgery, as most can be performed using the keyhole method. However, just because they are considered minimally invasive doesn’t make them any more successful or non-intrusive. It is invasive and even damaging to muscles, ligaments, spinal discs, spinal joints, or spinal nerves any time you cut into tissue. As such, they fail to provide long-term respite.
There are various types of minimally invasive spine surgery in Malaysia. The vast majority of patients would experience residual discomfort even if highly experienced surgeons in Europe or the United States did the surgical intervention. Moreover, most will require additional surgical interventions within 2-5 years following minimally invasive spine surgery, such as surgical decompression.
There are several types of minimally invasive spine surgery or spinal decompression surgery. We have listed them below:
Radiofrequency (RF) Ablation or Radiofrequency Neurotomy
Laminectomy or Laminotomy
Facetectomy or Spinal Joint Surgery
Foraminotomy
Partial Discectomy
Nucleoplasty
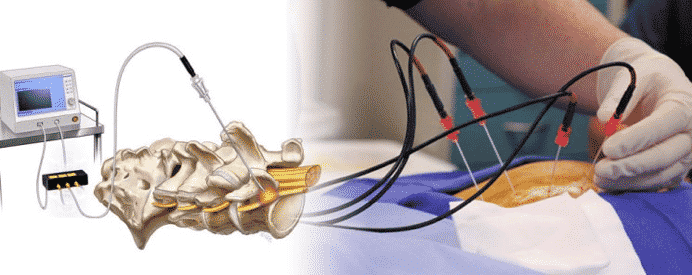
Radiofrequency Ablation (RFA) Or Radiofrequency Neurotomy For The Chronic Or Acute Spine Discomfort
Radiofrequency ablation (RFA) or radiofrequency neurotomy is a minimally invasive spine surgery. The primary goal of radiofrequency ablation or neurotomy is to destroy the nerves that senses discomfort. The term Neurotomy is descriptive of surgical interventions that cut or damage nerves that trigger symptoms of discomfort. Ablation is a general term meaning taking away or removal. In surgical scenarios, ablation applies to the surgical removal of tissue.
In short, Radiofrequency ablation and radiofrequency neurotomy are interchangeable terms used in the destruction of the innate or inherent functions of nerves. It is carried out through radiofrequency, which generates heat by radio waves. RF ablation has the most conflicting research when it comes to clinical success. Some call it an absolute failure, while others cite mild respite of discomfort temporarily.
All About Radiofrequency Ablation (RFA Or RF Ablation) Of The Spine:
Radiofrequency ablation or RF ablation is a minimally invasive spine surgical procedure that takes about one to two hours. The process requires using several specialized needles inserted in the vicinity of the discomfort-sensing nerve (medial branch nerve) in your lower back to destroy the nerve with heat. RFA or radiofrequency ablation for back patients is performed in an operating room under live X-ray. You will be positioned on your stomach, sedated through local anesthetics, and conscious during the procedure.
The surgeon will insert three to four needles after carefully assessing you, making sure that you are a candidate for the procedure. Once the needles are in place, the radiofrequency machine connected to the needles will start to send strong radio waves to the tip of the needles. Radio waves will heat the tip of these needles and burn the nearby tissues and nerves.
Most patients may experience increased discomfort and discomfort, and some may report an intense burning-like sensation similar to a severe sunburn in the area cared for. According to published reports, you should notice an improvement in symptoms two to three weeks following the procedure. However, RFA is not a cure. In fact, it may harm the nearby tissues, including the muscle that stabilizes your spine. To understand this better, we have outlined the functions of the medial branch nerve, which is a target of radiofrequency ablation surgery, below:
Sense discomfort in your spinal joints
Controls the ligaments of your spinal joints (medially)
The only nerve the innervates and controls the multifidus muscles
RFA for back pain: what it targets and why the details matter
What RFA aims to do: Radiofrequency ablation (RFA) uses heat at the tip of a small probe to create a tiny lesion next to the medial branch nerve. That nerve carries pain signals from the small joints of the spine (facet joints). By disrupting that signal, RFA can reduce joint-related back pain for some people often for a number of months.
What else the medial branch does: Besides pain signaling from the facet joints, the medial branch also provides a small motor supply to the multifidus, a deep stabilizing muscle that helps you stand upright, extend, side-bend, and rotate through the trunk. Because of that connection, RFA may also affect the multifidus in the treated area.
Why this matters: After medial branch RFA, fatty/atrophic change in the multifidus can occur on imaging for some patients and may be difficult to reverse. That’s why careful patient selection and a protect-the-muscle rehabilitation plan (spine-neutral motor control, graded loading, no provocative twisting early on) are important. Pain relief can also fade over time as nerves regrow, and some people consider repeat procedures another reason to plan strengthening around the stabilizers from the start.
Good questions to ask before RFA
Is my pain clearly coming from the facet joints (how was this confirmed)?
What result should I expect (pain, function, meds, return to work), and for how long?
What’s the plan to protect and retrain the multifidus after the procedure?
If relief is partial or short-lived, what are my next non-invasive options?
Therefore, many people first consider conservative, whole-spine care delivered non-invasively before procedures like RFA. For a plain-language overview, see this article on radiofrequency ablation (RFA) and conservative alternatives. (External educational resource; not medical advice. Discuss options with a registered clinician.)
A Better Alternative To Radiofrequency Ablation Surgery
Radiofrequency ablation or radiofrequency Neurotomy may provide you discomfort respite for 6-18-months at most suitable according to experts who studied this procedure!
So, why would you take the risk with methods known to fail in the long term? It’s a bit like silencing a warning light without fixing the engine: symptoms may quiet briefly, but the underlying issue can remain.
You wouldn’t because the problem will still be there, and in time, you will have more significant issues! The same applies to your body. Why would you cut or kill the nerve that warns you of a problem? Take our advice; short-term gains through invasive methods are wasteful at most suitable.
Our clinical teams are opposed to invasive procedures for the spine, including minimally invasive spine surgery. RF or Neurotomy, regardless of its level of invasiveness, is a procedure most suitable to be avoided. The harm inflicted on the joints and soft tissues outweighs even the most suitable possible scenario. In short, there are no shortcuts to getting better. Cutting away the nerves or killing them with heat or radio waves does not constitute a cure. Seek useful conservative care options before opting for this invasive procedure. Visit CSC’s award-winning chiropractor in Kuala Lumpur today and learn about the recommended comprehensive means of spine care.
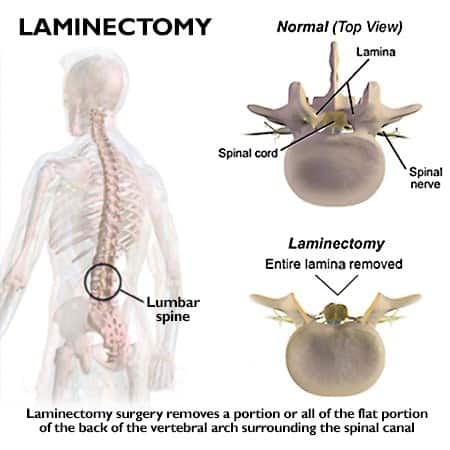
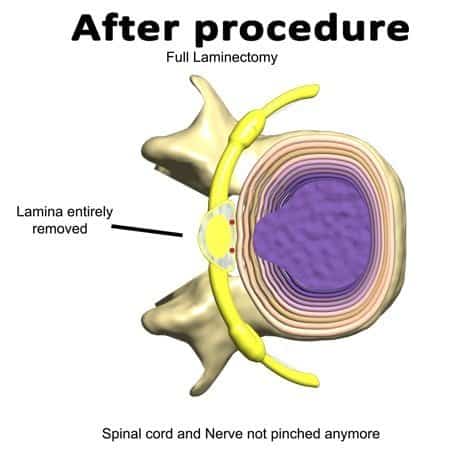
Spinal Decompression Through Laminectomy/Laminotomy
The lamina is the bony structure at the rear of the spine. They protect the spinal canal and enable the attachment of critical ligaments for spinal stability. Your spinal canal starts at the base of the skull and runs down to the tailbone. Laminectomy is a minimally invasive spine surgery that removes the lamina. Earlier, we mentioned that the lamina has the attachment point for a critical ligament. Ligamentum flavum is a highly specialized ligament that connects spinal segments through their laminal attachment points.
The ligamentum flavum limits excessive motion and has the contractile ability to reposition the spine into proper alignment following a flexion or forward bending. Repetitive traumatic events, poor posture, and prolonged sitting can lead to hypertrophy of the ligamentum flavum. Hypertrophy of the ligamentum flavum can increase the chance of developing spinal canal stenosis.
A laminectomy is performed not because the lamina has issues but rather due to the thickening of the ligamentum flavum. In reality, this procedure is performed to remove the thickened or hypertrophied ligamentum flavum. The surgeon may remove a part of the lamina (partial laminectomy) or all of it. In the old days, they removed the whole lamina.
In recent times, they remove only parts to avoid excessive instabilities that often arise from a laminectomy. Surgeons refer to this as minimally invasive spine surgery, as it can be performed through a keyhole method of surgical intervention. According to published research, patients that opt for a laminectomy often require a second or third surgical intervention.
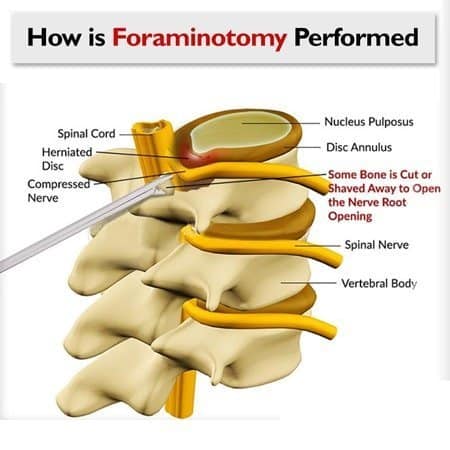
Decompression Of Spine Performed Through A Foraminotomy
Spinal nerves originate from the spinal cord. As they leave the cord, they pass through a passageway. The passageway provides protection and an exit point for the spinal nerves. These passageways are termed intervertebral foramina or foramen. But, the foramina are not a passage just for the nerves.
Other structures also pass through this opening, including the spinal artery, veins, and sinuvertebral nerve (the major discomfort-sensing nerve for spinal discs, spinal joints, and joint ligaments). The spinal discs’ borders are formed by the spinal discs, spinal bones (vertebral bodies) anteriorly, and spinal joints (facets) posteriorly. Arthritic or degenerative changes of spinal discs, vertebral bodies, and facet joints will result in the foramina’s narrowing.
Narrowed spinal foramina (vertebral foramina) are classified as stenotic. The term used to describe such conditions is called foraminal stenosis. The narrowed foramina (foraminal stenosis) compress the spinal nerves and vessels within the passageway (vertebral foramen).
Foraminotomy is the process of removing portions of the bony walls (pedicels of the top of facets or parts of vertebral bones), spinal discs, or both. Furthermore, the cutting of spinal discs and pedicles on top of facets may lead to instabilities. As a result, most patients who undergo a foraminotomy need additional surgical interventions such as a nucleoplasty, laminectomy, discectomy, or spinal fusion in the future.
Nucleoplasty: What Recent Studies Show About Benefits and Risks
Some studies report limited benefit for nucleoplasty (and related techniques such as IDET) in carefully selected patients, and sham-controlled trials of IDET did not show advantage over placebo at 6 months. That doesn’t mean no one improves; it means expectations should be cautious, risks and alternatives weighed, and conservative plans optimized before disc procedures are considered..
The authors reported the average patient discomfort level before nucleoplasty at 6.7 (on a Visual Analog Scale or VAS of 1-10, with 10 being excruciatingly severe). Nine months after nucleoplasty, discomfort levels were documented at 5.6, equating to a 10% decrease in discomfort. In other words, nucleoplasty has a failure rate of 100% because none of the nine patients were rendered discomfort-free. They only improved by 10% on average! As such, the authors concluded that nucleoplasty, with or without IDET, may have limited clinical benefit based on the outcomes observed in their study.
Nucleoplasty is a form of discectomy where portions of the spinal discs are removed from the inside of your spinal discs.
Percutaneous discectomy or nucleoplasty is a minimally invasive spine surgery that we adamantly oppose. Generally speaking, we oppose most surgical procedures performed in the absence of targeted non-surgical therapy. However, our reservation toward nucleoplasty remains, as studies have not consistently demonstrated clear clinical benefits. Notably, one study found that sham (placebo) nucleoplasty showed similar outcomes to the actual procedure.
Are There Different Types Of Nucleoplasty For The Spine?
Two approaches are described in the literature: nucleoplasty alone and nucleoplasty combined with IDET. Evidence of benefit is limited and inconsistent; selection and conservative optimization first are recommended.
Nucleoplasty without intradiscal electrothermal therapy (IDET)
Nucleoplasty with intradiscal electrothermal therapy (IDET)
The process of inserting a catheter (introducer) at the center of the spinal disc is damaging, but cooking it through electrothermal means blows the mind. However, most troubling is the motive behind this rootless procedure’s continued use in light of its documented failures!
A randomized, double-blind study from the Department of Orthopedics at the Royal Adelaide Hospital in South Australia concluded no differences between the nucleoplasty with IDET and the sham IDET procedure. The study was published in the Spine Journal.
It included 58 patients; of the 58 patients, 38 were cared for through an actual IDET method, and 19 were cared for with a fake or sham IDET method. The fake surgery (sham) was provided in much the same manner as the real one, except for the inner disc material’s cutting and heating. If your surgeon is recommending nucleoplasty, you need to read this research article first.
Six months after the procedures, there were no differences between the real and fake spine operations.
Your surgeon’s hope with a nucleoplasty is to remove the nerve pressure caused by spinal disc herniation or disc bulge, better known as a slipped disc or slip disc. Regardless of their hopes of clinical achievements, nucleoplasty renders your surgically cared for disc unstable. The instabilities result from the cutting of the inner tissues of the spinal disc. Just because you have a disc herniation, you don’t need to cut it apart from the inside. Let CSC’s clinical teams assist your non-invasive recovery from joints, ligaments, or slipped disc.
IDET (heated disc) vs placebo: what a gold-standard trial found
IDET heats the outer disc (annulus) to try to shrink/“seal” tears; nucleoplasty is different but related it removes/disrupts inner disc material (nucleus). In a rigorous randomized, double-blind, placebo-controlled trial of IDET for chronic discogenic low back pain (patients had 1–2 symptomatic levels with annular tears and had already tried conservative care), 57 people were randomized (38 IDET; 19 sham). At 6 months, no patient in either group met the study’s predefined “successful outcome”, and standard measures (Oswestry Disability Index, SF-36, etc.) did not improve meaningfully with IDET compared with placebo. There were no permanent neurologic complications reported.
What this means for you: if you’re being offered IDET or a nucleus-targeting procedure like nucleoplasty, ask how “success” will be defined for you (pain, function, meds, return to work), what benefit is realistically expected, and what non-invasive options remain. This trial suggests IDET did not outperform placebo at 6 months in a carefully selected group, so it’s reasonable to seek a second opinion and review conservative, image-informed, low-force care before choosing a disc procedure.
Citation: Freeman BJC, Fraser RD, Cain CMJ, Hall DJ, Chapple DCL. A randomized, double-blind, controlled trial: intradiscal electrothermal therapy versus placebo for the treatment of chronic discogenic low back pain. Spine (Phila Pa 1976). 2005;30(21):2369-2377; discussion 2378. doi:10.1097/01.brs.0000186587.43373.f2.
Discectomy Is The Type Of Operation That Removes The Spinal Disc In Part Or Totally.
The spinal discs are the separators, connectors, shock absorbers, and stabilizers of the spine that provide mobility and weight-bearing. Poor posture, prolonged sitting, and repetitive traumatic events lead to degenerative changes that impact the health of spinal discs.
A degenerated spinal disc is a weak structure that is unable to provide efficient loadbearing and mobility. In time, a degenerated disc can succumb to stresses of daily life, causing the spinal disc to tear, bulge, herniate, or rupture. A bulging disc or a herniated disc is better known by its layperson term, slipped disc or slip disc.
As the spinal disc fibers protrude, bulge, or herniate beyond their normal boundary, they can push or pinch the spinal nerve or spinal cord.
Spine surgeons often recommend cutting portions or all of the discs in their entirety, depending on the severity of protrusions. Although there is sufficient data that reports the retraction of spinal discs through conservative means, surgeons still prefer to perform microdiscectomy or total discectomy of patients with slipped discs.
A partial discectomy usually accompanies laminectomy, facetectomy, and foraminotomy. Partial discectomy can be performed through the keyhole method and, as such, is considered by surgeons as minimally invasive spine surgery. A complete discectomy is usually accompanied by spinal fusion. Regardless of the type, discectomy is not a cure. Patients may continue to suffer from varying degrees of discomfort after discectomy.
The cutting of spinal discs will lead to instability in the spinal segments adjacent to the surgical site. As such, patients are often advised to exhaust their conservative route before considering the surgical options.
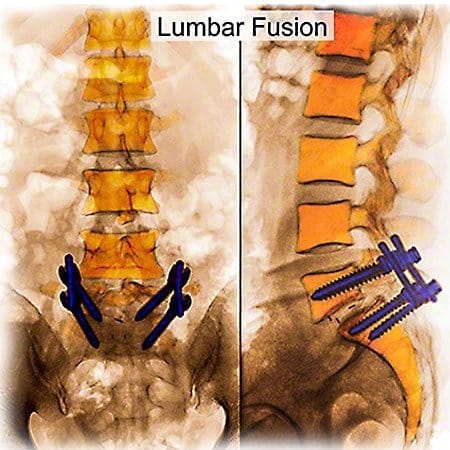
Spinal Fusion: An intervention For Severe Cases Or For Failed laminectomy (laminotomy), Facetectomy, Foraminotomy, Nucleoplasty & Partial Discectomy.
Spinal fusion is a surgical intervention that has been around for decades. It was the go-to method of spine surgery for most surgeons. In spinal fusion, the surgeon attempts to fuse spinal bones through implants, a bone graft, or a combination of the two. Fusion aims to stop mobility or motion in hypermobile, unstable, or excessively damaged segments. There are various methods of spinal fusion, including minimally invasive spine surgery.
Each type of method has its merits and disadvantages. In some patients, the surgical method is performed from the front, the back, or the front and back. It is often harvested from the patients’ hip or a synthetic source if the bone graft is used. In spinal fusion, a surgeon removes the facet joints and the spinal disc.
They may pack the void with spacers or a bone graft. Also, screws may be used to hold the implant and spacer (hardware) in place. The bone graft will join one or more spinal segments into a single solid mass. With fusion, there can be a loss of mobility. Restricted motion is a common cause of additional stress on segments adjacent to the fused vertebrae.
Spinal fusion may increase mechanical stress on nearby segments (adjacent-segment changes), which can contribute to problems over time in some patients. Not everyone develops this; risk varies with factors like number of levels fused, alignment, and activity.
Spinal fusions are common in patients who continue to suffer from discomfort after laminectomy (laminotomy), facetectomy, foraminotomy, or partial discectomy. Our advice is if you have had surgery and failed to provide the help you were seeking, visit one of our centers.
If the first surgery didn’t help, pause before the second
Fusions are often proposed after a laminectomy, foraminotomy, or partial discectomy hasn’t relieved symptoms. If one operation hasn’t delivered the result you hoped for, it’s important to re-evaluate before signing up for another. Each additional surgery is more complex: there’s more scar tissue, the spine’s mechanics change, and reported re-operation rates rise in several cohorts.
In short, repeating the same approach without a clear new diagnosis rarely improves the odds. This is why we and many clinicians who want the good long-term outcome encourage exhausting a structured, non-surgical plan first. Don’t wait until surgery feels like the only option; that’s often when the risks of post-surgical back issues climb.
Smarter next steps (before surgery #2 or #3)
Reassess the cause: correlate symptoms with a fresh clinical exam and available imaging; confirm the actual pain generator(s).
Try a time-boxed conservative plan: gentle, non-rotatory care with clear checkpoints (e.g., visits 5/10/15) and measurable goals.
Get two opinions: one surgical and one non-surgical. If both agree surgery is necessary or there’s a true emergency proceed informed.
(Educational guidance, not medical advice. Decisions should follow a thorough assessment by a registered clinician.)
How Long Does It Take To Recuperate From The Operation?
Recovery from spine surgery can take 3 to 4 months. However, three to four months is the minimum. For some patients, it can take six months or more. The recovery rate depends on your overall health, the skill of your surgeon, follow-up care, home care, and your activities of daily living. In short, you will need to give it some time.
Symptoms can recur after surgery for some people. Rates vary by diagnosis, procedure type, rehabilitation, and individual factors another reason to plan follow-up care carefully and set patient-meaningful goals.
Complete recovery to a point where you are free of all symptoms might be rare. Unless, of course, the surgical intervention is for relatively minor conditions that would have done well with conservative care.
You should seek a second and third opinion before considering surgery. For preferred results, consult a second surgeon and a nonsurgical spine caregiver like a chiropractor or a physiotherapist before opting for spine surgery. We will be happy to provide this service for you.
How Successful Is The Back Operation? Let’s See What Research On The Spine Journal Reported.
According to a published research article in the renowned Spine Journal, fusion causes spinal stenosis, disc herniations, and instabilities next or adjacent to the surgically fused segment. In other words, patients who were operated on through spine fusion surgery developed spinal disc problems in healthy segments before surgery.
Spine surgery (laminectomy, foraminotomy, discectomy, nucleoplasty, or spinal fusion) can reduce discomfort if successful, but it will also hamper your spine’s ability to function normally. In time, the operated-on segment or those near the surgical site will decay or degenerate faster. Spinal fusions have the highest rate of degenerative changes in the good ones. We have provided the recap of that research below:
All fifty-eight patients acquired spinal stenosis, disc herniation, or disturbance in a section next to previously asymptomatic or healthy spinal segments. In short, spinal fusions could result in damage and symptoms that arise from segments that are adjacent to the operated site.
Impact Of Cervical Laminectomy
Another published research on the clinical outcomes of 64 cervical laminectomy noted abnormal changes in spinal curvatures in 36% of patients. Also, 14% of the patient cases studied resulted in reversed cervical curvatures or kyphotic curves two years post-surgery. Furthermore, two of the 64 patients needed additional surgeries. Additional surgeries were needed two years following the first surgery to address the instabilities caused by laminectomy.
Unfortunately, this study did not elaborate on the level of discomfort, function, symptoms, or quality of life following surgery. Also, the study only reviewed cases 2-years post-surgical intervention. We are confident that had they examined patient cases at five years and seven years (post-surgical study), the reported statistics would undoubtedly be much higher among those needing a second or even a third operative procedure. Nonetheless, from the limited information gathered, one could persuasively argue that laminectomy has a success rate of 50%.
The most astonishing report on the long-term success or outcomes of a lumbar fusion surgery comes from research conducted by the Ohio Bureau of Workers’ Compensation records. We have provided a link to your review’s abstract of a historical cohort on surgical spinal fusion.
Why Spine Surgery Sometimes Falls Short
Clinicians sometimes use the term failed back surgery syndrome (FBSS) when pain returns or never fully settles after an operation. That doesn’t mean surgery never helps many people do well. It means there are biomechanical and diagnostic reasons why relief can be incomplete.
What can go wrong and why:
Load shifts to other levels. Fusing or reshaping one segment can increase stress on the discs and joints above/below (often called adjacent-segment changes), which may become irritated over time.
Scar and sensitivity. Healing can create scar tissue around nerves (epidural fibrosis) or leave tissues more reactive, keeping symptoms going even after the original compression is treated.
Muscle shutdown and deconditioning. Pain and incision protectiveness can inhibit deep stabilisers (e.g., the multifidus). Without a plan to rebuild them, support stays weak and movement stays guarded.
Target mismatch. Imaging may show several findings, but not all findings cause pain. If the true “pain generator” isn’t addressed, symptoms can persist.
Movement/posture drivers remain. Habitual flexed sitting, repeated end-range bending, or poor hip mechanics can keep loading the same segment, regardless of what was done surgically.
More surgery ≠ better odds. Re-operations are typically more complex (more scar tissue, altered mechanics). That’s why a careful re-assessment is vital before “surgery #2 or #3.”
Minimally invasive ≠ consequence-free. Smaller incisions still alter mechanics and tissues; they can help selected cases, but they are not immune to the issues above.
Practical takeaway: If you’re not facing an emergency, exhaust a measured, non-invasive plan first calm-first care, image-informed decisions, and staged rehab that rebuilds stabilisers and movement control. If surgery is needed (or already done), pair it with a targeted rehabilitation plan and clear checkpoints so progress is tracked and gaps are addressed early.
(Educational information only. Decisions should follow a thorough assessment by a registered clinician.)
European Spine Journal on Spine Surgery
An article in the European Spine Journal reported on the eliminating of a patient discomfort or symptoms through invasive spinal decompression methods by experienced surgeons at 90% two months after the operation. The failure rate drops to 75% after five years with medication.
A study in the European Spine Journal reported that after lumbar decompression (laminectomy, foraminotomy, facetectomy, or partial discectomy), 90% of patients still had leg symptoms at 2 months. At 5 years, 75% continued to report symptoms, often requiring medication; 25% reported no leg pain. In the same cohort, 24% later had a second surgery (fusion), and a smaller subset underwent a third (5-year lumbar decompression outcomes (Eur Spine J, 2010).
The paper nevertheless described the operations as “successful” highlighting a key gap between research success (any measurable improvement) and patient success (low pain, good function, fewer meds, return to normal life). In other words, symptom reduction ≠ symptom resolution.
Any decrease in patients’ symptoms backed the author’s claims of surgical successes. In other words, any evidence of improvement was deemed as the success achieved. You can download and read this research below:
Spine Fusion Failure Was Related To Permanent Disabilities In 74% Of Workers In The U.S. State Of Ohio.
Researchers examined the clinical outcomes of 1,450 patients using the Ohio Bureau of Workers’ Compensation database. The researchers specifically targeted patients with a diagnosis of disc degeneration, disc herniation, or radiculopathy. Let’s define what radiculopathy is first.
Radiculopathy is discomfort that runs down one or both limbs due to nerve compression or nerve damage. Patients complaining of radiculopathy may experience discomfort, tingling (pins and needles), burning sensations, and weakness in one or both limbs.
Those with neck-related radiculopathy may experience symptoms in the upper and lower extremities. Radiculopathy involving the lower back mainly impacts the lower buttocks and legs.
Now, let’s get back to the research article. Researchers divided the database into two equal groups, surgical and non-surgical. It is important to note that both groups had patients who suffered from the same diagnosis and severity. In short, of the 1,450 cases, 750 were operative patients, and the remaining 750 received non-invasive care. The researcher compared the clinical outcomes in each group after two years. Keep in mind that patients in both groups had identical complaints. Although they were similar, the recovery and overall success were not the same.
Only 26% of the injured workers that were operated on returned to work. The remaining 74% of fusion patients were considered medically disabled and as such, unfit to continue their work-related activities.
The published statistics equate to a resounding failure rate of 74% for surgical patients. Had the surgery been successful, surely the patients would have returned to work! Now, let’s see how the non-surgically cared for patients did. The non-surgical group got targeted physical therapy (physiotherapy) methods.
Of the 750 physiotherapy patients, 67% returned to work within two years. The study offers clear evidence that spine surgery may not allow the patient to return to an active life post-surgery. Additionally, the research establishes the impact of clinically targeted physiotherapy methods as opposed to surgery.
Why Should You Seek A Second Opinion From A Non-Surgical Provider When Your Surgeon Recommends A Procedure?
We live in a world where the opinions and recommendations of neurosurgeons and orthopedic surgeons are not questioned. Simply put, when spine surgeons recommend surgery, patients follow their advice.
There is nothing wrong with putting your trust in the doctors and surgeons who care for you. After all, you willingly went seeking their professional opinion.
But, as with any medical recommendation, you may want to seek a second and even third option in non-life-threatening situations. Orthopedic surgeons and neurosurgeons spend years learning surgical methods for the spine.
They are physicians that specialize in spine surgery. In short, their research, training, and continuing education are all concentrated on perfecting their surgical skills and knowledge. But, by their surgical background, little time is spent on non-surgical means. As such, most are unaware of recent developments in the targeted non-surgical care of the spine.
We recommend getting a surgical second opinion and a non-surgical second opinion. So, get a non-surgical second opinion from chiropractors and physiotherapists who specialize in targeted research-based clinical methods of spine care. In short, visit our center. Our experts have provided non-surgical spine care at an unparalleled level of success to thousands. We have helped even those who have had failed surgical interventions.
Why Should You Seek Out Second Opinions From Chiropractors When The Surgeon Has Recommended An Operation For The Spine?
A spine surgeon’s clinical focus is on surgical interventions. A chiropractor’s focus is entirely dedicated to non-surgical methods. Chiropractors help with focused non-surgical spine care, helping with spine-related conditions daily, weekly, monthly, and yearly. In short, a highly experienced clinical chiropractor is the recommended individual to visit for non-surgical second opinions.
Chiropractors and physical therapists, or physiotherapists, have been caring for the spine for over a century. For obvious reasons, a surgeon’s education and training are focused on surgical methods of care. Likewise, a chiropractor or physiotherapist (physical therapist) spends years learning non-surgical methods. However, it must be said that surgeons, chiropractors, and physiotherapists may hold degrees but differ. Some surgeons excel more than others!
The same holds for chiropractors and physiotherapists. So, care must be taken when choosing one. Please don’t shy away or be afraid to ask your neurosurgeon, orthopedic surgeon, chiropractor, or physiotherapist about their education, training, expertise, and experience.
Ask them about their personal experiences in similar conditions and results achieved. Question them on surgical and non-surgical methods. Ask them about the time they spend researching surgical and non-surgical techniques of spine care. Don’t be afraid; it is your spine, health, and long-term well-being at stake.
So, speak up and get as much information from each specialty about your options. Doing so will enable you to make a better-informed decision.
Non-Surgical Spinal Decompression Therapy Conservative Care Options for the Neck & Back
NSD Therapy® is an alternative, non-invasive method of spine care.. It is a multi-faceted spine care system rendered by research-based chiropractors, and clinical physiotherapy is provided through manual and integrated spine-specific technologies. If your surgeon is recommending spine surgery, NSD Therapy® can help. Visit us today to discover the recommended alternative to spine surgery.
Our clinical teams of Chiropractors and Physiotherapists use spine-specific methods and technologies such as the decompression therapy, Laser, and flexion-distraction to help your recovery for neck and back issues. Best of all, the care you get from us is non-invasive. We have cared for many across our center who sought our help with their slipped disc, neck discomfort, and back discomfort.
NSD Therapy®: a gentle, customizable, non-surgical plan
NSD Therapy® is one of our non-surgical options for selected spine conditions. It’s a gentle, non-rotatory, team-delivered protocol that aims to calm irritated tissues and improve movement and, for some people, may reduce the likelihood of needing injections or surgery. We first introduced NSD Therapy® at our Bukit Damansara (Kuala Lumpur) center and now offer it at several CSC locations. To ask whether it suits your case, call 03-2093 1000.
How we tailor NSD Therapy®
Stepwise assessment: history, movement and posture screen, segment-by-segment palpation, and a focused neurological check.
Image-informed planning: our registered clinicians review your MRI images (T1/T2) in addition to the radiologist’s report. We look for the exact level(s) involved, annular tears, Modic/end-plate changes, facet irritation, soft-tissue signal suggesting inflammation, and muscle quality (e.g., fatty infiltration). We also consider tissue depth (how many cm below the skin) to choose modalities that can actually reach the target safely.
Calibrated, comfort-first care: forces, angles, and session length are adjusted to your tolerance; no forceful twisting or end-range “cracking.”
Measured progress: clear goals and checkpoints; we modify the plan based on your response.
What we may use (case-by-case)
Angle-controlled spinal decompression to reduce load at the involved level(s).
Flexion–distraction (brief, non-rotatory).
SOT blocking + Activator for precise, low-force alignment cues.
High-intensity laser (Class IV) when deeper penetration is needed (dose-controlled).
Therapeutic ultrasound applied with a smooth, gel-cushioned glide (not pressure massage).
Focused shockwave at low settings for superficial tender points when appropriate.
Electrotherapy and spine-neutral motor control to rebuild support without flaring symptoms.
What NSD Therapy® is not
Not a single machine or one-size-fits-all protocol.
Not aggressive stretching, deep paraspinal pressure, or rotatory thrusts.
Not planned from a report alone we correlate your exam findings with the actual MRI images to decide what’s safe and likely to help.
Educational information only; not a diagnosis or medical advice. Care decisions should follow a thorough assessment by a registered clinician. Individual results vary.
Who shouldn’t delay a surgical opinion (or urgent assessment)
Most backs settle with measured, non-invasive care. Still, get urgent hospital assessment or a surgeon’s review if you notice:
Progressive leg/foot weakness or new foot drop needs urgent imaging and specialist review within 24–48 hours (same day if worsening fast). Depending on findings, conservative care may still resume but don’t delay the assessment.
Bowel or bladder changes, or saddle numbnessemergency: go to the ER now (possible cauda equina).
Recent major trauma or suspected fracture no manual therapy until imaged (X-ray/CT/MRI first).
Fever, chills, or unexplained weight loss with back pain requires medical work-up to rule out infection or tumor.
For non-urgent cases with clear nerve compression that don’t improve after a time-bound, well-run conservative plan, a surgical opinion is reasonable to discuss options.
Author:
Yama Zafer, D.C., with an educational background in physiotherapy and chiropractic from Cleveland Chiropractic University in Kansas City, has dedicated nearly three decades to the fields of physiotherapy and chiropractic; read more about Y. Zafer.
Peer-Reviewed Medical References:
Deyo RA, Mirza SK, Martin BI. Back pain prevalence and visit rates: estimates from U.S. national surveys, 2002. Spine. 2006;31(23):2724-2727.
Chou R, Deyo R, Friedly J, et al. Noninvasive Treatments for Low Back Pain. Agency for Healthcare Research and Quality (US); 2016.
Fritz JM, Childs JD, Wainner RS, Flynn TW. Primary care referral of patients with low back pain to physical therapy: impact on future health care utilization and costs. Spine. 2012;37(25):2114-2121.
Weinstein JN, Lurie JD, Tosteson TD, et al. Surgical vs nonoperative treatment for lumbar disk herniation: the Spine Patient Outcomes Research Trial (SPORT) observational cohort. JAMA. 2006;296(20):2451-2459.
Chou R, Huffman LH. Nonpharmacologic therapies for acute and chronic low back pain: a review of the evidence for an American Pain Society/American College of Physicians clinical practice guideline. Ann Intern Med. 2007;147(7):492-504.
Bronfort G, Haas M, Evans R, Leininger B, Triano J. Effectiveness of manual therapies: the UK evidence report. Chiropr Osteopat. 2010;18:3.
Cherkin DC, Deyo RA, Sherman KJ, et al. A randomized trial comparing acupuncture, simulated acupuncture, and usual care for chronic low back pain. Arch Intern Med. 2009;169(9):858-866.
Last Updated:
Last updated by Y. Zafer, D.C., September 1, 2025.: Spine Surgery Risks & Optional Non-Invasive Care.
Spine Surgery & Non-Invasive Care – FAQs
What does “successful” mean in studies and how is that different from what patients expect?
In clinical papers, any measurable improvement can count as success (e.g., a small drop in a pain or disability score). For most people, success means low enough discomfort to live normally, fewer meds, better sleep/walking tolerance, and a return to work or sport. Your page explains this gap and shows why procedures labeled “successful” in journals may still leave some with persistent symptoms. Agree on patient-meaningful targets with your clinician (pain ≤3/10 most days, walk/sit 30–60 minutes, med step-down, no new deficits) and review them at set checkpoints (e.g., weeks 2/4/8).
When is spine surgery usually considered?
True red flags: progressive neurological loss, bowel/bladder changes, cauda equina signs. Clear structural compression with matching symptoms that does not improve after a well-run, time-bound course of conservative care. Instability, deformity, fracture, infection, or tumor where operative care is standard. Outside these, many improve with a calm-first, non-invasive plan.
What are the main risks and limitations of common procedures (laminectomy, foraminotomy, discectomy, fusion)?
All surgery is invasive “minimally invasive” still cuts tissue. Reported issues include dural tears, nerve irritation/injury, infection, and adjacent-segment problems. Your page summarizes research where decompression procedures often left residual leg symptoms, and where fusion cohorts showed higher reoperation/complication and opioid-use rates and lower return-to-work in specific populations. Outcomes vary by person, procedure and surgeon; that’s why shared definitions of success and clear follow-up plans matter.
Are “minimally invasive” procedures more successful?
Smaller incisions don’t guarantee better long-term results. Your content notes that even keyhole approaches can change spinal mechanics, create scar tissue, and may still require additional surgeries within a few years for some people. Decisions should weigh imaging-symptom match, conservative response, and personal goals not incision size alone.
If my first surgery didn’t help, what should I do before considering a second or third?
Reassess the cause: fresh clinical exam + available imaging to confirm the pain generator(s). Time-boxed conservative plan: gentle, non-rotatory care with checkpoints (e.g., visits 5/10/15) and measurable goals. Two opinions: one surgical and one non-surgical. If both point to surgery or there’s an emergency proceed informed. Repeating the same approach without a new diagnosis rarely improves the odds; risks typically rise with each operation.
What does a good non-invasive plan look like and when might I feel a change?
Start calm and precise: no forceful twisting or end-range “cracking” during inflammatory phases; correlate exam with MRI images (not just the report); use dose-controlled modalities (e.g., angle-controlled decompression, brief flexion–distraction, high-intensity laser, ultrasound, focused shockwave at low settings when indicated). Add movement re-education and core control only when tissues tolerate loading. Many notice steadier days in a few weeks when flare drivers are reduced, with progress reviewed at planned checkpoints. Individual results vary.
What is NSD Therapy® and who might it suit?
NSD Therapy® is a gentle, team-delivered protocol not a single machine. It starts with stepwise assessment (history, movement, segment palpation, focused neuro check) and image-informed planning (your clinicians review T1/T2 MRI images alongside the report to identify levels, tears, Modic/end-plate and facet changes, soft-tissue signals, and muscle quality). Care is calibrated to tissue depth and tolerance (no rotatory thrusts), and may include angle-controlled decompression, brief flexion–distraction, SOT/Activator alignment cues, high-intensity laser, therapeutic ultrasound, focused shockwave for superficial tender points, and electrotherapy with spine-neutral motor control. It’s considered for selected spine conditions after individual evaluation.
We need a bit more information before we could give advice.
What was the diagnosis before the surgical intervention? Did you have one or multiple surgeries?
When did the paralysis occur? Was it rapid onset or progressive in nature?
What types of surgical intervention did you have for the injuries sustained four years ago?
We understand that you may not want to post personal information on the blog. If you wish, please email us directly ([email protected]). You can post here as well, but others will be able to read your comments as well. It might be better to email us your history and concerns that you have. We will need to review the required information before giving you advice about the available alternatives.
Thank you for sharing your situation regarding PIVD at L4-L5 with nerve compression affecting both legs for the past five years. Given that you posted this comment on our blog post titled “All About Surgery,” it appears you might be considering surgical options as a solution to your ongoing discomfort.
While surgery can be an effective intervention for severe cases of nerve compression, I strongly recommend exploring comprehensive conservative treatment approaches before proceeding with surgery. At CSC, we specialize in a multi-disciplinary approach that integrates chiropractic care, physiotherapy, and focused rehabilitation. This combination has been successful in alleviating symptoms similar to yours and, in some instances, we have even been able to reverse the effects of a protruded intervertebral disc by as much as 90% without the need for invasive procedures.
Our conservative treatment methods aim to relieve nerve compression naturally, improve spinal alignment, and strengthen the supporting musculature. These non-surgical approaches are designed to address the root causes of pain and dysfunction, providing lasting relief and potentially reducing the need for surgery. Many patients find significant improvement in their symptoms and overall spinal health through these treatments.
Before making a decision about surgery, I encourage you to explore all conservative options available. If you are interested in a detailed evaluation to see if our integrative approach could be effective for your condition, please do not hesitate to contact us. You can reach us via WhatsApp at +(60)17-269-1873 or visit our center to discuss your condition in more detail.
We’re here to help you explore every possible avenue for relief and recovery, ensuring that surgery is considered only after all other treatments have been thoroughly pursued.











I’m a paraplegic. I injured my spine 4 years ago. I have surgical instruments in L4 and T6.
Dear Christopher,
We need a bit more information before we could give advice.
What was the diagnosis before the surgical intervention? Did you have one or multiple surgeries?
When did the paralysis occur? Was it rapid onset or progressive in nature?
What types of surgical intervention did you have for the injuries sustained four years ago?
We understand that you may not want to post personal information on the blog. If you wish, please email us directly ([email protected]). You can post here as well, but others will be able to read your comments as well. It might be better to email us your history and concerns that you have. We will need to review the required information before giving you advice about the available alternatives.
PIVD L4 L5 nerve compression on both sides for the last 5 years.
Hello,
Thank you for sharing your situation regarding PIVD at L4-L5 with nerve compression affecting both legs for the past five years. Given that you posted this comment on our blog post titled “All About Surgery,” it appears you might be considering surgical options as a solution to your ongoing discomfort.
While surgery can be an effective intervention for severe cases of nerve compression, I strongly recommend exploring comprehensive conservative treatment approaches before proceeding with surgery. At CSC, we specialize in a multi-disciplinary approach that integrates chiropractic care, physiotherapy, and focused rehabilitation. This combination has been successful in alleviating symptoms similar to yours and, in some instances, we have even been able to reverse the effects of a protruded intervertebral disc by as much as 90% without the need for invasive procedures.
Our conservative treatment methods aim to relieve nerve compression naturally, improve spinal alignment, and strengthen the supporting musculature. These non-surgical approaches are designed to address the root causes of pain and dysfunction, providing lasting relief and potentially reducing the need for surgery. Many patients find significant improvement in their symptoms and overall spinal health through these treatments.
Before making a decision about surgery, I encourage you to explore all conservative options available. If you are interested in a detailed evaluation to see if our integrative approach could be effective for your condition, please do not hesitate to contact us. You can reach us via WhatsApp at +(60)17-269-1873 or visit our center to discuss your condition in more detail.
We’re here to help you explore every possible avenue for relief and recovery, ensuring that surgery is considered only after all other treatments have been thoroughly pursued.
Best regards,