


Meniscus Tear Care in KL: Gentle Non-Surgical Options
A meniscus tear is one of the most common knee issues affecting walking, stair use, squatting, turning, and sports-related movement. The meniscus is the cartilage cushion inside the knee that helps absorb load and allows smoother joint motion. When it becomes strained, worn, or torn, people often notice swelling, stiffness, joint-line discomfort, catching, or difficulty fully straightening the knee.
For broader guidance on knee symptoms, swelling, instability, cartilage wear, and ligament-related concerns, visit our main page: Knee Care in KL & PJ at CSC. Many people looking for meniscus care in KL without surgery or injections also benefit from understanding how meniscal tears may overlap with ACL, PCL, cartilage, and long-term knee stability concerns.
Meniscus Tear Care in KL: Non-Surgical Options
Meniscus tear care in KL should begin with a careful assessment of the knee, not with a fixed routine. The meniscus helps distribute load between the thigh bone and shin bone, so symptoms may appear during walking, stairs, squatting, twisting, kneeling, or getting up after sitting.
At Chiropractic Specialty Center®, meniscus-related knee concerns may be reviewed through joint movement checks, meniscus-related movement tests, ligament screening, kneecap tracking review, walking assessment, and muscle control testing around the hip, knee, ankle, and foot.
Non-surgical care may include chiropractic joint mobilization, registered physiotherapy, soft tissue methods, guided rehabilitation, activity modification, walking review, and exercise progression when appropriate. The care plan should depend on the tear type, symptoms, movement findings, imaging when available, and whether locking, swelling, instability, or giving-way is present.
Surgery may still be discussed in some cases, especially when the knee has true locking, an unstable tear pattern, major trauma, or symptoms that do not respond to appropriate conservative care. For many non-obstructive or degenerative meniscus-related concerns, structured rehabilitation is often considered before invasive options.
Key Points About Meniscus Tear Care in KL
- The meniscus helps distribute load, guide movement, and reduce friction between the thigh bone and shin bone.
- Each knee has two menisci: the medial meniscus on the inner side and the lateral meniscus on the outer side.
- Meniscus symptoms may include swelling, stiffness, joint-line discomfort, catching, clicking, locking, or difficulty fully straightening the knee.
- Twisting, pivoting, deep squatting, stairs, and getting up after sitting may make meniscus-related symptoms more noticeable.
- Some tear patterns, such as flap tears or bucket-handle tears, may interfere with knee movement and need closer assessment.
- Tear location matters because the outer meniscus has better blood supply than the inner meniscus.
- Meniscus findings may overlap with ACL, PCL, collateral ligament, cartilage, tendon, kneecap tracking, or walking mechanics.
- Non-surgical care may include joint mobilization, registered physiotherapy, soft tissue methods, guided rehabilitation, and activity modification when appropriate.
- Surgery may be discussed when true locking, significant instability, trauma-related injury, or persistent mechanical symptoms are present.
- For Meniscus Tear Care in KL, assessment should guide the next step rather than relying on the MRI label alone.
Meniscus Tear Guide: Symptoms, Locking, Recovery & Care Options in KL
What the Meniscus Is and Why It Matters for Knee Stability
The meniscus is a strong, rubbery cartilage structure inside the knee that helps cushion the joint and guide smooth movement. Each knee has two menisci — the medial meniscus on the inner side and the lateral meniscus on the outer side.
The medial meniscus is commonly described as C-shaped, while the lateral meniscus is more rounded and closer to a circular profile. Together, they sit between the thigh bone (femur) and the shin bone (tibia), helping distribute body weight during standing, walking, stair use, squatting, and sports-related movement.
Rather than being flat, the meniscus has a wedge-like, cup-forming shape that helps the femur sit more securely over the tibia. This shape plays an important role in how the knee bends, rotates, and absorbs load during daily movement.
The outer edge is generally thicker and has better direct blood supply, while the inner portion is thinner and receives nutrients mainly from the joint fluid. This difference may influence how different tear patterns respond over time.
Beyond shock absorption, the meniscus also helps with joint stability, load distribution, movement control, and protection of the cartilage surfaces.
Because the meniscus helps guide how the knee moves, certain tear patterns — especially flap tears and bucket-handle tears — may shift during bending and lead to locking, catching, or difficulty straightening the knee.
Why a Meniscus Tear Can Cause Locking, Catching, or Difficulty Straightening the Knee
One of the most common complaints with a meniscus tear is a locking or catching sensation in the knee. Some people describe the knee as getting stuck during walking, stair use, squatting, or when standing up after sitting.
This happens because a torn part of the meniscus may temporarily interfere with how the thigh bone and shin bone glide over each other during movement. In certain tear patterns, such as flap tears or bucket-handle tears, a loose segment of meniscal tissue may shift during bending and create a catching sensation or make the knee feel as if it cannot fully straighten.
Twisting, pivoting, and turning while the foot is planted often make this symptom more noticeable. When locking becomes more frequent, it may suggest a tear pattern that needs closer clinical evaluation.
How Meniscus Tear Care May Be Structured
A meniscus tear may affect more than one part of the knee. Meniscus changes can influence joint loading, kneecap tracking, cartilage surfaces, ligaments, tendons, muscle control, and walking mechanics.
For that reason, care is often structured in stages. The first stage usually focuses on understanding the tear pattern, swelling, range of motion, locking, instability, and how the knee responds during daily movement. The next stage may focus on restoring knee motion, improving muscle control, and reducing repeated strain during walking, stairs, bending, and squatting.
A meniscus care plan should not focus only on the tear. The hip, ankle, foot, walking pattern, and lower-limb control often influence how much load reaches the knee..
Depending on the findings during assessment, a structured program may include several approaches that focus on different tissues and functions:
- High-intensity laser therapy may be used when deeper joint tissues and soft tissue recovery are part of the care plan.
- Therapeutic ultrasound may be considered for more superficial tissues such as the collateral ligaments, patellar tendon, and soft tissue structures around the knee.
- Shockwave therapy may be used in selected cases involving tendon-related changes or chronic tissue irritation around the knee.
- Electrotherapy may be included as part of movement re-education and symptom management.
- Manual soft tissue and trigger point work may focus on the quadriceps, hamstrings, calf muscles, iliotibial band, and lateral stabilizers that influence knee mechanics.
- Guided rehabilitation and exercise help improve strength, balance, and control through the hip, knee, and ankle chain.
- Gentle non-rotatory chiropractic knee mobilization may be considered when joint mechanics and alignment need attention.
Depending on assessment findings, care may include chiropractic knee joint mobilization, registered physiotherapy, soft tissue methods, guided rehabilitation, walking review, and selected technology-assisted physiotherapy when appropriate. Exercise should usually be progressed gradually, beginning with motion and control before heavier strengthening is added.
Chiropractic Joint Mobilization for Meniscus-Related Knee Concerns
Meniscus-related knee concerns may sometimes be linked with altered joint movement, kneecap tracking, hip control, ankle mobility, or walking mechanics. When assessment findings suggest joint restriction or movement imbalance, gentle chiropractic joint mobilization may be considered as part of a broader care plan.
The purpose is not to force the knee or twist the joint. The focus is on how the tibiofemoral joint, patellofemoral joint, surrounding soft tissues, and lower-limb mechanics work together during daily activity.
At CSC, chiropractic joint mobilization may be coordinated with registered physiotherapy, guided exercise, and soft tissue methods when appropriate. The care plan should be guided by symptoms, movement findings, imaging when available, and whether the knee has swelling, locking, instability, or restricted movement.
Video: How Knee Load, Meniscus Stress & Movement Mechanics Affect Recovery
Understanding a meniscus tear often requires looking beyond the cartilage itself. Knee load is influenced by how force transfers through the hips, pelvis, ankle, foot, and surrounding muscles during walking, stairs, squatting, and exercise. In the video below, Yama Zafer explains how movement mechanics, cartilage load, meniscus function, and guided exercise principles may influence longer-term knee stability and recovery.
This video is especially useful for readers who want to better understand why symptoms may keep returning even after rest and how weight transfer through the lower body may affect meniscal stress.
An 18-minute educational walkthrough on knee load, meniscus stress, cartilage mechanics, and guided exercise principles presented by Yama Zafer, D.C
Key Moments From the Video
- 00:00 Why knee symptoms develop and what may be driving repeated strain
- 00:41 How the knee functions as a weight-transfer joint
- 01:52 Meniscus and cartilage load during movement
- 03:15 How alignment changes may affect knee wear patterns
- 04:50 Uneven loading, stiffness, and movement warning signs
- 05:40 When imaging such as X-ray or MRI may be discussed
- 06:55 Conservative care and movement-based options
- 08:00 Knee warm-up and controlled movement exercises
- 08:58 Tubing and range-of-motion drills
- 10:12 Wall squat mechanics and form
- 11:53 Inner and outer thigh muscle strengthening
- 14:38 Gym-based knee rehabilitation movements
- 15:53 Quadriceps and hamstring balance
- 17:35 Leg press and adductor machine tips
Physiotherapy for Meniscus Tear Care in KL
Physiotherapy for meniscus tear care focuses on movement, control, strength, balance, and walking mechanics. A meniscus-related knee concern may change how the quadriceps, hamstrings, calf muscles, hip muscles, and foot position work during daily activity.
A physiotherapy plan may include range-of-motion work, soft tissue methods, balance training, walking review, hip and knee strengthening, and progressive exercises for stairs, squatting, and activity return. The order of exercise matters because adding load too early may increase knee stress when swelling, locking, or poor control is still present.
Technology-assisted methods such as high-intensity laser, ultrasound, electrotherapy, or shockwave may be considered only when assessment findings suggest they are appropriate. These methods should be part of a structured plan, not a stand-alone solution.
For Meniscus Tear Care in KL, physiotherapy should match the tear pattern, symptoms, activity goals, and knee response during movement.
What Long-Term Studies Show About Exercise and Meniscus Recovery
Structured rehabilitation is often explored first in many non-obstructive knee and meniscus-related symptoms, and this approach is strongly supported by long-term clinical research.
A randomized clinical trial published in JAMA (2018) by van de Graaf and colleagues compared early arthroscopic surgery with structured physical therapy for non-obstructive meniscal tears and found that exercise-based rehabilitation provided comparable knee function outcomes in many patients.
This was further reinforced by the five-year ESCAPE follow-up study published in JAMA Network Open (2022) by Noorduyn and colleagues, which reported that exercise-based physical therapy remained non-inferior to arthroscopic partial meniscectomy for patient-reported knee function over five years.
These findings support beginning with structured rehabilitation, movement correction, strengthening, and load-management strategies before invasive procedures are considered in many degenerative meniscal cases.
Key Clinical Research on Meniscus Recovery Pathways
- van de Graaf VA, Noorduyn JCA, Willigenburg NW, et al. Effect of Early Surgery vs Physical Therapy on Knee Function Among Patients With Nonobstructive Meniscal Tears. JAMA. 2018;320(13):1328-1337.
- Noorduyn JCA, van de Graaf VA, Willigenburg NW, et al. Effect of Physical Therapy vs Arthroscopic Partial Meniscectomy in People With Degenerative Meniscal Tears: Five-Year Follow-up of the ESCAPE Randomized Clinical Trial. JAMA Netw Open. 2022;5(7):e2220394.
Related Knee Structures & Recovery Guides to Explore Next
A meniscus tear does not always happen alone. Depending on how the knee was injured, nearby ligaments, cartilage surfaces, and movement mechanics may also be involved. The pages below can help you better understand related knee structures, instability patterns, and recovery pathways that commonly overlap with meniscal injuries.
- PCL Injury Care & Gentle Knee Rehabilitation
for back-of-knee instability and dashboard-type injuries - ACL & Knee Ligament Injury Care
when twisting injuries or sports-related instability are present - Knee Care in KL & PJ
for a broader guide to knee symptoms and joint function - Runner’s Knee & Front Knee Symptoms
when stair discomfort or kneecap-related symptoms are more noticeable - Knee Arthritis & Degenerative Knee Changes
for age-related wear, cartilage thinning, and stiffness - Knee Exercise & Rehabilitation Guide
for strengthening, balance, and movement recovery
The two most common invasive care for a torn meniscus are steroid injections or arthroscopic knee surgery for meniscus. Published studies in the New England Journal of Medicine and the Journal of Radiology have questioned steroid injections and refuted the clinical benefits of arthroscopic knee surgery. This article provides in-depth information about the meniscus, meniscal tears, types, symptoms, remedies, and care options.
The Knee’s Meniscus
The meniscus is a pair of essential, tough, resilient rubber-like structures made of cartilage that helps form a hinge joint at the knee by separating your thigh bone (femur) from the shinbone (tibia). There are two menisci (plural for meniscus) in each knee:
- The Medical Meniscus
- The Lateral Meniscus
The medial and lateral menisci disperse the body’s weight, provide shock absorbance, reduce friction, and enable smooth movements at the knee joint. The medial meniscus is a “C” shaped structure, while the lateral meniscus is more circular.
Medial meniscus:
- It covers 50% of the medial tibial plateau
- It is immobile
- The commonly injured meniscus
- Firmly attached to the tibial plateau
Lateral meniscus:
- Cover 70% of the lateral tibial plateau
- This is the mobile meniscus
- Associated with a Discoid meniscus
- Anterior & posterior horns are closer, terminating near the ACL
Meniscal damage, injury, and discomfort are too common and can impact the young and elderly. Actual meniscal tears are the most common cause of meniscal discomfort in younger individuals. In the elderly, degenerative artists known as wear and tear arthritis is the leading cause of meniscal discomfort. Regardless of the reason, meniscal tears, injuries, and tears are repairable without surgery.
Nutrient Availability
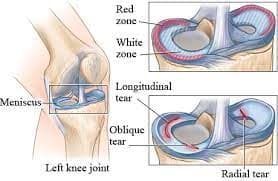
- The peripheral 1/3 of the meniscus is vascular which is classified as a “Red Zone” or “red-red zones”
- The middle 1/3 is classified as a mixed zone “Red-White Zone” sometimes called the “pink zone”
- The inner 1/3 is vascular but nourished by the synovial fluids and classified as the “White Zone” or “white-white zone”
Meniscus Tear Medial (Medial Meniscal Tear)
Medial meniscus and ACL tear happen when a flexed knee is twisted inwards (medially) with the foot firmly planted on the ground. The medial meniscus is a “C” shaped immobile structure covering nearly 50% of the medial tibial plateau. It is the most commonly injured meniscus. Most medial meniscal tears occur when the knee is twisted while the foot is firmly planted on the floor. Moreover, medial meniscus tears always accompany damage to the ACL.
The ACL (Anterior Cruciate Ligament) gets injured when the medial meniscus is torn because the medial meniscus gives rise to the ACL. Therefore, if the force of the knee injury is sufficient to hurt the meniscus, it will also damage or tear the ACL. And by the same token, an Anterior Cruciate Ligament injury or tear will always present with a medial meniscal tear.
Suppose you are diagnosed with a meniscal tear. In that case, you should avoid arthroscopic knee surgery as it was found inefficient in a double-blind clinical trial published in the New England Journal of Medicine. Medial meniscus tears can heal if you get focused physiotherapy combined with knee-and-meniscus-specified chiropractic care methods.
Meniscus Tear Lateral (Lateral Meniscal Tear)
The lateral meniscus is more of a circular-shaped mobile meniscus attached to the lateral tibia plateau. The lateral meniscus covers about 70% of the lateral tibial plateau. The lateral meniscus will be larger and cover most of the lateral tibial plateau on rare occasions. A larger lateral meniscus is referred to as a “Discoid” meniscus. You can have a discoid meniscus and not know and never experience any discomfort.
Lateral meniscal injuries are not as common as medial meniscal injuries because the lateral meniscus is mobile. A lateral meniscus tear occurs when the knee joint is rotated or twisted outwards. Also, an injured or torn lateral meniscus will often accompany a damaged Posterior Cruciate Ligament or PCL.
Torn Meniscus The ACL & PCL
Patients with torn medial or lateral meniscus must also have their cruciate ligaments (ACL & PCL) carefully assessed. MRI assessment is the gold standard for diagnosing ACL, PCL, and meniscal issues. However, MRI reports are rarely detailed. Often time, they leave out co-conditions and injuries that are mild. Therefore, if you have been diagnosed with ACL, PCL, or meniscal tears, you will need your doctor to carefully review your MRIs for co-tears in other structures, including the medial and lateral collateral ligaments and the ACL & PCL ligaments.
Are There Difference Meniscal Tear Types?
The menisci (medial and lateral meniscus) assist in mobility and provide shock absorbance as it separates and cushions the knee joint-degenerative changes and injuries lead to a damaged or torn meniscus. A torn or damaged meniscus can be excruciatingly uncomfortable.
Meniscus tears are classified into six categories or types:
- Intrasubstance or the incomplete meniscal tear
- Radial tear
- Horizontal tear
- Bucket-handle tear
- Complex tear
- Flap tear
Can a Meniscus Tear Improve Without Surgery?
Some meniscus-related symptoms may improve without surgery, especially when the tear is degenerative, non-obstructive, or not causing true locking. Structured rehabilitation may help improve knee motion, muscle control, walking tolerance, and daily function in selected cases.
Healing potential depends on several factors, including tear location, tear type, blood supply, age, activity level, swelling, knee stability, cartilage condition, and whether nearby structures such as the ACL, PCL, or collateral ligaments are involved.
The outer portion of the meniscus has better blood supply than the inner portion, which may influence how different tear patterns respond over time. The inner portion receives more support from joint fluid and usually has less direct blood supply.
Surgery may still be discussed when the knee has repeated true locking, a displaced tear, major trauma, or symptoms that remain limiting after appropriate conservative care. The best next step depends on assessment findings, imaging, and how the knee behaves during daily movement.
Importance Of Meniscus’s Red, Red-White, And White Zones & What They Mean?
The medial and lateral menisci are divided into three zones depending on nutrient and blood flow:
The “RED” zone or outer zone of the meniscus is the most vascularized zone where healing occurs faster.
“RED-WHITE,” the middle, or the pink zone, is in the middle. The “Red-White” zone has less direct blood flow than the “Red” zone, as such healing occurs at a slower pace when compared to the RED zone.
“WHITE,” or the innermost part of the meniscus, is void of direct blood supply. The “white” zone of the meniscus fulfills its nutrient requirements from the synovial fluids.
What Are The Six Possible Complication Of Torn Meniscus Left Untreated?
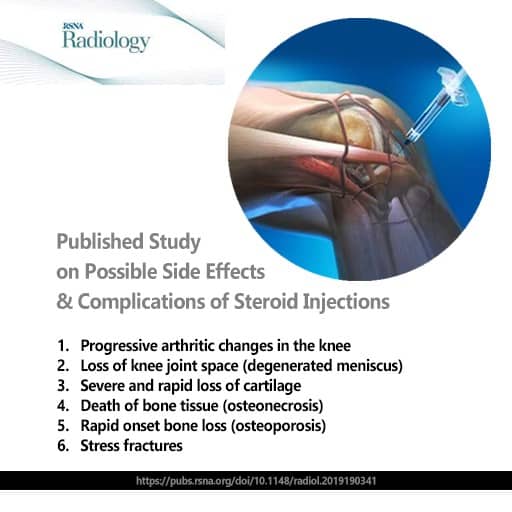
If you have been diagnosed with a meniscal tear, you need chiropractic combined with physiotherapy care to help you heal faster. The dangers of an untreated meniscal tear include premature degenerative and arthritic changes in the knee joint. As mentioned in earlier parts, torn meniscus also presents with some degree of ACL or PCL damage. A common complication of a torn meniscus is PCL or ACL ligament tears. Here are some additional complications when a meniscal tear is neglected or poorly treated:
- Degeneration of the femoral condyles
- Degeneration of the meniscus and cartilage
- Osteoarthritis along the edges of the knee joint or at attachment points of ACL & PCL
- Flap tears of the meniscus are more common in long-standing chronic meniscal issues.
- Development of Baker’s Cyst
- Thighbone and leg bone damage (subchondral bone damage, degeneration, and edema)
Complications for untreated meniscus tears can be severe and life-altering; therefore, heed the warning and get your meniscal tear treated before complications arise.
Meniscus Tear Symptoms: Locking, Swelling, Clicking, and Stiffness
Meniscus tear symptoms may vary depending on the tear pattern, location, and whether nearby structures are involved.
Common symptoms may include:
- Swelling after walking, stairs, squatting, or sports activity
- Joint-line discomfort on the inner or outer side of the knee
- Clicking, catching, or locking sensations
- Difficulty fully straightening or bending the knee
- Discomfort during twisting, pivoting, kneeling, or deep squatting
- Stiffness after sitting or resting
- A feeling that the knee may give way
- Reduced confidence during stairs or uneven ground
Repeated locking, giving-way, sudden swelling after injury, or inability to bear weight should be assessed promptly.
What Is The Mechanism Of Discomfort In Damaged Or Torn Meniscus?
Innervate the outer 1/3 of the anterior and posterior horns of the medial and lateral meniscus. Published studies have documented nerves innervation of the menisci. A study published in the Journal of Arthroscopy reported findings of research conducted on twenty-three cadaver knee tissues studied under a microscope. The authors said the meniscus has nociceptive nerve innervation (discomfort-sensing nerves) and the outer 1/3 In both horns of the lateral and medial meniscus.
Direct meniscus discomfort:
The synovium, ligaments, and menisci of the knees have discomfort-sensing nerves. Degenerative changes and tears trigger these nerves and transmit the sensation of discomfort. Additionally, a 2016 study published in the Annals of the Rheumatic Diseases compared healthy meniscal tissues from asymptomatic donors to meniscal tissues of damaged and symptomatic knee patients. The authors of this study noted a significant increase in nerve proliferation in damaged missus tissues instead of meniscus tissues studied from healthy asymptomatic donors.
The study in the Annal of the Rheumatic Diseases suggests that meniscal damage leads to the sensation of discomfort and a significant increase in the number of discomfort-sensing nerve fibers or cells.
Subchondral meniscus-related discomfort:
The subchondral bone of the knee joint is the layer directly under the cartilage that covers the condyles of the knee joint. The cartilage has no nerve supply, but the subchondral bone is richly innervated. A torn meniscus exposes the tibial surface to the condyles of the femur. Direct contact between the femoral condyles and the tibial plateau results in cartilage degeneration on the femoral condyles and the tibial plateau. Progressive degenerative changes on the femoral condyle’s cartilage or the cartilage attached to the tibial plateau cause irritation and damage to the subchondral bone and, as such, irritate the subchondral network of nerves, causing discomfort in the knee joint.
Non-Surgical Meniscus Tear Care in Kuala Lumpur
Non-surgical meniscus tear care in Kuala Lumpur may include several methods depending on the tear pattern, symptoms, imaging findings, and daily movement needs.
A structured plan may include:
- Registered physiotherapy for range of motion, strength, balance, and walking mechanics
- Chiropractic joint mobilization when knee joint movement or tracking needs review
- Soft tissue work for quadriceps, hamstrings, calf, iliotibial band, and hip-related muscle tension
- Guided rehabilitation exercises progressed according to knee response
- Activity modification for stairs, squatting, kneeling, twisting, and walking distance
- Footwear, hip control, and ankle mobility review when lower-limb mechanics affect knee load
The aim is to improve movement control and daily function while monitoring symptoms such as swelling, locking, instability, and walking tolerance.
Personalized Meniscus Exercise & Rehab Programs
Exercise and rehabilitation for meniscus care should never follow a one-size-fits-all model. At CSC in KL, our rehab programs are tailored to the individual based on the location and classification of the meniscal tear—whether horizontal, radial, or complex. A well-designed exercise plan must support meniscal healing while preventing further microtrauma or degeneration.
Our rehab strategies begin with joint unloading techniques and non-weight-bearing mobility drills, then progress to isometric and closed-chain strength work. Special attention is given to restoring knee flexion-extension balance and ensuring correct muscle activation patterns—especially in the vastus medialis, gluteus medius, and intrinsic foot stabilizers.
Balance and proprioception play a key role in protecting a healing meniscus. Using controlled stability drills and low-impact resistance tools, our team focuses on improving reflexive muscle coordination to reduce joint shear and control rotational stress during movement.
Most importantly, exercises are progressed based on tissue response and not fixed timelines. Whether the injury is recent or chronic, a progressive rehab strategy aligned with biomechanical feedback leads to improved mobility and function without aggravating the joint.
Combined Chiropractic & Physiotherapy for Meniscus Injuries
Integrating chiropractic with physiotherapy offers a multi-dimensional strategy for meniscus recovery. This combined approach, available at CSC centers in Kuala Lumpur, addresses both joint alignment and soft tissue mechanics—creating a cohesive path toward recovery for medial and lateral meniscus injuries.
Chiropractors focus on improving knee joint congruency and reducing abnormal loading through precise, non-twisting adjustments. Meanwhile, physiotherapists manage soft tissue adaptation, neuromuscular control, and movement retraining. When used together, this method addresses both cause and consequence of meniscus-related dysfunction.
Patients receive coordinated care that starts with clinical imaging and biomechanical analysis. Once the type and location of the tear are identified, our team develops a care plan that includes targeted joint mobilization, fascia release, instrument-assisted therapy, and functional loading programs. Modalities like laser or shockwave may be included for deep-tissue repair, especially in avascular meniscal zones.
Rather than viewing meniscus recovery as isolated to one structure, our approach considers the full kinetic chain—from hip and spine stability to ankle mobility. This combined methodology promotes better outcomes while avoiding high-impact movements or unnecessary procedures.
Steroid Injections for Knee and Meniscus Symptoms: What to Discuss
Steroid injections are sometimes discussed for knee symptoms, especially when swelling or inflammatory joint irritation is present. However, the decision should be made carefully with a qualified medical professional, especially when the concern involves the meniscus, cartilage, or long-term joint health.
Some studies have raised questions about repeated corticosteroid injections and their possible relationship with cartilage changes or later joint findings in selected groups. This does not mean every injection is harmful or inappropriate, but it does mean the decision should be individualized.
For meniscus-related symptoms, many people first explore non-surgical care such as registered physiotherapy, guided rehabilitation, activity modification, walking review, and joint mobilization when appropriate. The right path depends on symptoms, imaging, swelling, function, and whether locking or instability is present.
When Meniscus Surgery May Be Discussed
Meniscus surgery may be discussed when symptoms suggest a tear pattern that is interfering with knee mechanics. This may include repeated true locking, a displaced bucket-handle tear, significant trauma, or symptoms that remain limiting after a structured course of appropriate non-surgical care.
Surgical options may include partial meniscectomy, meniscus repair, or, in selected cases, meniscus reconstruction. The decision depends on tear type, tear location, age, activity needs, tissue quality, knee stability, cartilage condition, and whether other structures such as the ACL or PCL are involved.
Many degenerative or non-obstructive meniscus tears are often approached first with structured rehabilitation. Long-term studies have reported that exercise-based physiotherapy can provide comparable knee function outcomes to arthroscopic partial meniscectomy in selected patients.
The decision should be made after proper clinical assessment, imaging review, and discussion with an appropriate medical professional.
Meniscectomy For Torn Meniscus
Meniscectomy can be total or partial. It is commonly prescribed to patients with a radial meniscal tear in the white-white zone (meniscal zones with no direct blood supply) or flap tears. Moreover, it can be an open knee surgery or arthroscopically and may be combined with meniscal reconstruction surgery. However, you should avoid all forms of meniscectomy as it can lead to degenerative changes, requiring additional surgical interventions.
We encourage efficient multi-disciplinary non-surgical care that target the meniscus tear before any surgical intervention. Short-term results are good, but the long-term effects are unfavorable as they always lead to degenerative and arthritic conditions. Therefore, meniscectomy should be performed only when you have exhausted an efficient means of therapy that combines physiotherapy with meniscus-specific chiropractic care.
Arthroscopic Surgery For Meniscal Repair
The clinical outcomes of a double-blind study involving arthroscopic surgery for meniscus failed to show any benefit at all. Also, a separate study with over 4,600 participants showed that arthroscopic surgeries were associated with eventual knee replacements due to degenerative changes induced by arthroscopic procedures. Therefore, we discourage all forms of arthroscopic surgery for the meniscus as it can lead to more harm.
However, in the event you still want information, we have provided a brief description of surgical repair of a torn meniscus:
Meniscus tear repair through open or arthroscopic surgery is exclusively performed on meniscal tears that are recent or acute and located within the peripheral walls of the meniscus in the vascularized red-red zones of healthy younger patients. This surgical intervention is often recommended for:
- Horizontal tears in younger athletes
- Root tears
- Radial tears and, at times, tears in red-white zones
Meniscal Reconstruction Surgery
Meniscal reconstruction surgery is often recommended for patients with total or partial meniscectomy. Meniscal reconstruction surgery aims to fill the gap resulting from a meniscectomy. The procedure is accomplished through one of the two commonly used methods:
- Meniscal scaffolds
- MAT (Meniscal Allograft Transplantation)
Arthroscopic Surgery For Meniscus Tear
Some surgeons use the old slogan for meniscal tears, “If it’s torn, cut it out & throw it away!’ However, recent literature advises against cutting or removing the meniscus, and as such, a newer slogan is now encouraged, “Do everything to Save the meniscus!”
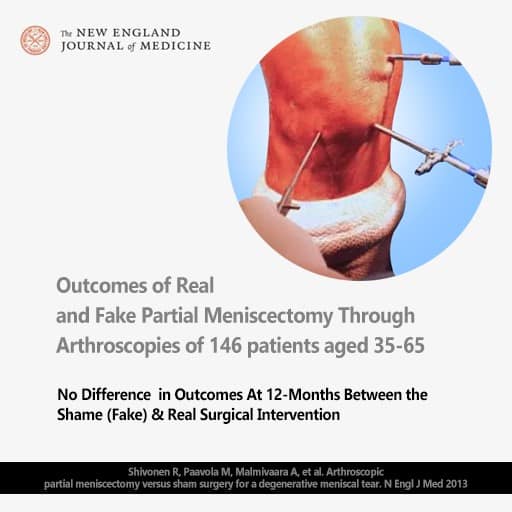
The New England Journal of Medicine published a study of the efficiency of meniscal surgery. What sets the study apart from others is that it published the results of a randomized double-blind sham-controlled partial meniscectomy (arthroscopic meniscal tear surgery) of 146 patients aged 35-65. The outcomes call into question the use of arthroscopic surgery for patients with a torn meniscus.
The Outcome:
No Difference in Outcomes At 12-Months Between the Shame (Fake) & Real Surgical Intervention.
Another eye-opening study published in the peer-reviewed Journal of Osteoarthritis and Cartilage reported that patients that received meniscal tear surgery had a 300% increased chance of getting a TKR (total knee replacement) within 2 years of the meniscal surgery.
This study suggests that it is prudent for people who suffer from knee discomfort resetting from arthritis or meniscal tears to consider getting focused knee care at Chiropractic Specialty Center® from our chiropractors and physiotherapists combined before considering knee surgery.
Simple Meniscus Tear Care Tips Before Assessment
Simple steps may help reduce repeated knee stress while waiting for assessment. These steps should not replace clinical review, especially when swelling, locking, giving-way, or difficulty walking is present.
Helpful starting points may include:
- Avoid twisting or pivoting on the affected knee
- Limit deep squatting or kneeling if symptoms increase
- Use stairs slowly and avoid rushing down steps
- Keep walking distances manageable
- Avoid sudden increases in exercise or sports activity
- Use short periods of rest when swelling increases
- Keep early exercises gentle until the knee response is understood
- Track symptoms such as locking, swelling, clicking, or giving-way
Seek assessment promptly if the knee locks, gives way, swells after injury, or becomes difficult to fully straighten.
Knee Discomfort Care In Kuala Lumpur For Knee Discomfort Including Torn Meniscus, Knee Arthritis, Torn Ligaments & Damaged Cartilage
Chiropractic Specialty Center® (CSC) in Kuala Lumpur provides holistic clinical knee care for all knee problems causing discomfort, instability, or weakness. CSC’s knee discomfort care protocols are integrative and combined care methods from the top-rated award-winning team of holistic clinical physiotherapists with evidence-based chiropractors in Kuala Lumpur.
Holistic clinical physiotherapy pertains to knee discomfort and knee injuries and targets injured and degenerated need tissues, including the cartilage, ligaments, tendons, muscles, and meniscus, by modern therapeutic devices such as high-intensity laser therapy and targeted shockwave therapy to help your recovery. Evidence-based chiropractic starts with a thorough assessment that helps formulate a customized holistic approach to help the injured knee recover faster. Yama Zafer, D.C. (Doctor of Chiropractic), Has manage thousands of knee discomfort patients for over 25 years. His clinical knowledge and expertise have helped many recover from knee injuries and knee with lasting comfort. Learn more about our knee discomfort care for meniscus, ACL, and arthritis by visiting us today.
Author
“Meniscus Tear Care in KL: Gentle Non-Surgical Options” was prepared with input from Yama Zafer, D.C., who has U.S. training in chiropractic and physiotherapy and nearly three decades of experience in spine, joint, and movement-focused care in Malaysia; read more about Y. Zafer on his official bio page.
Peer-Reviewed References for Meniscus Tear Care in KL
- Makris, E. A., Hadidi, P., & Athanasiou, K. A. (2011). The knee meniscus: Structure-function, pathophysiology, current repair techniques, and prospects for regeneration. Biomaterials, 32(30), 7411–7431.
- Logerstedt, D. S., Scalzitti, D. A., Bennell, K. L., Hinman, R. S., Silvers-Granelli, H., Ebert, J., Hambly, K., Carey, J. L., Snyder-Mackler, L., Axe, M. J., McDonough, C. M., & Irrgang, J. J. (2018). Knee pain and mobility impairments: Meniscal and articular cartilage lesions revision 2018. Journal of Orthopaedic & Sports Physical Therapy, 48(2), A1–A50.
- van de Graaf, V. A., Noorduyn, J. C. A., Willigenburg, N. W., Butter, I. K., de Gast, A., Mol, B. W., Saris, D. B. F., Twisk, J. W. R., Poolman, R. W., & ESCAPE Research Group. (2018). Effect of early surgery vs physical therapy on knee function among patients with nonobstructive meniscal tears: The ESCAPE randomized clinical trial. JAMA, 320(13), 1328–1337.
- Noorduyn, J. C. A., van de Graaf, V. A., Willigenburg, N. W., Scholten-Peeters, G. G. M., Kret, E. J., Mulder, B. M., Mol, B. W., Saris, D. B. F., Twisk, J. W. R., Poolman, R. W., & ESCAPE Research Group. (2022). Effect of physical therapy vs arthroscopic partial meniscectomy in people with degenerative meniscal tears: Five-year follow-up of the ESCAPE randomized clinical trial. JAMA Network Open, 5(7), e2220394.
- Krych, A. J., Reardon, P. J., Johnson, N. R., Mohan, R., Peter, L., Levy, B. A., & Stuart, M. J. (2017). Non-operative management of meniscal tears. Clinics in Sports Medicine, 36(1), 93–109.
- Brophy, R. H., Matava, M. J., & Smith, M. V. (2012). The role of arthroscopy in the treatment of degenerative meniscus tears. Current Reviews in Musculoskeletal Medicine, 5(3), 180–186.
- Englund, M., Guermazi, A., & Lohmander, S. L. (2009). The role of the meniscus in knee osteoarthritis: A cause or consequence? Radiologic Clinics of North America, 47(4), 703–712.
- Englund, M., Roos, E. M., & Lohmander, L. S. (2003). Impact of type of meniscal tear on radiographic and symptomatic knee osteoarthritis: A sixteen-year follow-up of meniscectomy with matched controls. Arthritis & Rheumatism, 48(8), 2178–2187.
- Sihvonen, R., Paavola, M., Malmivaara, A., Itälä, A., Joukainen, A., Nurmi, H., Kalske, J., Järvinen, T. L. N., & Finnish Degenerative Meniscal Lesion Study Group. (2013). Arthroscopic partial meniscectomy versus sham surgery for a degenerative meniscal tear. New England Journal of Medicine, 369(26), 2515–2524.
- Abram, S. G. F., Judge, A., Beard, D. J., & Price, A. J. (2020). Adverse outcomes after arthroscopic partial meniscectomy: A study of 700,000 procedures in the national Hospital Episode Statistics database for England. The Lancet, 395(10230), 1099–1109.
Last Updated
Last updated May 7, 2026: “Meniscus Tear Care in KL | Non-Surgical Knee Guide” was reviewed for clarity, local relevance, meniscus tear education, non-surgical knee care structure, and chiropractic with physiotherapy care guidance.
Meniscus Tear FAQ: Symptoms, Surgery, and Non-Surgical Care in KL
The questions below cover the most common concerns people have about meniscus tears, including locking, swelling, stair use, recovery time, tear types, and when surgery may be discussed. These answers are written to help readers better understand how meniscal injuries affect knee movement and what non-surgical care options may be explored.
What does a meniscus tear usually feel like?
A meniscus tear often causes swelling, stiffness, joint-line discomfort, and pain with twisting or squatting. Some people also notice catching, clicking, or difficulty fully straightening the knee.
Can a meniscus tear cause the knee to lock?
Yes. Certain tear patterns, especially bucket-handle tears and flap tears, may shift inside the knee and temporarily block normal movement, causing a locked knee or catching sensation.
Why does twisting make a meniscus tear worse?
Twisting places rotational stress through the meniscus. When the foot is planted and the body turns, the torn tissue may become compressed or displaced, making symptoms more noticeable.
Can a meniscus tear improve without surgery?
Some meniscus-related symptoms may improve without surgery, especially in non-obstructive or degenerative cases. The outcome depends on tear type, tear location, swelling, stability, activity level, and rehabilitation progress.
How long does meniscus rehabilitation usually take?
Recovery varies depending on the tear type, severity, and whether nearby ligaments are involved. Mild tears may improve over several weeks, while more complex tears may require a longer rehabilitation period.
What is the difference between medial and lateral meniscus tears?
The medial meniscus is located on the inner side of the knee and is more commonly injured. The lateral meniscus sits on the outer side and is more mobile.
Can stairs make a meniscus tear worse?
Yes. Going up and especially down stairs often increases knee bending load and may make swelling, discomfort, and catching symptoms more noticeable.
Can a meniscus tear happen together with ACL or PCL injuries?
Yes. Meniscus tears commonly occur with ACL and sometimes PCL injuries, especially after sports trauma, twisting injuries, or sudden directional changes.
When is surgery usually discussed for a meniscus tear?
Surgery may be discussed when symptoms persist, when there is repeated locking, or when the tear pattern significantly interferes with normal knee movement.
When should I get my knee assessed?
You should seek an assessment early if you have swelling, locking, catching, instability, or difficulty walking after a knee twist, fall, sports injury, or sudden pain episode.
Can a meniscus tear improve without surgery?
Yes. In many non-obstructive and degenerative meniscal cases, structured rehabilitation and exercise-based physiotherapy may help improve knee function, movement control, and symptom patterns without immediate surgery. Long-term clinical studies have reported comparable outcomes between rehabilitation and arthroscopic partial meniscus surgery in selected cases.
Is physiotherapy better than meniscus surgery?
For many degenerative meniscal tears without true locking, structured physiotherapy may be considered a preferred first step. Long-term randomized clinical studies have shown that exercise-based rehabilitation may provide outcomes comparable to surgery for knee function in many patients.
What Long-Term Studies Show About Exercise and Meniscus Recovery
Surgery is generally considered only after a thorough clinical assessment and after structured conservative care has been explored where appropriate.
Many knee symptoms, including kneecap tracking issues and some meniscus-related patterns, may improve with targeted rehabilitation, movement correction, and guided strengthening.
Procedural options may be discussed when symptoms involve persistent true locking, unstable tear patterns, significant structural disruption, or when well-planned conservative care does not lead to meaningful improvement.
What does a meniscus tear usually feel like?
A meniscus tear may cause swelling, stiffness, joint-line discomfort, clicking, catching, locking, or discomfort during twisting, squatting, stairs, or getting up after sitting.
Can a meniscus tear cause the knee to lock?
Yes. Certain tear patterns, such as bucket-handle tears or flap tears, may shift inside the knee and interfere with movement, making the knee feel locked or stuck.
Why does twisting make meniscus symptoms worse?
Twisting places rotational load through the knee. When the foot is planted and the body turns, the meniscus may become compressed or irritated, especially when a tear is present.
Can a meniscus tear improve without surgery?
Some meniscus-related symptoms may improve without surgery, especially in non-obstructive or degenerative cases. The outcome depends on tear type, tear location, swelling, stability, activity level, and rehabilitation progress.
How long does meniscus rehabilitation usually take?
Rehabilitation time varies. Mild symptoms may improve over several weeks, while more complex tears, swelling, instability, or related ligament findings may require a longer rehabilitation period.
What is the difference between medial and lateral meniscus tears?
The medial meniscus is located on the inner side of the knee and is commonly involved in twisting injuries. The lateral meniscus is on the outer side and moves more freely during knee motion.
Can a meniscus tear happen with ACL or PCL injury?
Yes. Meniscus tears may occur together with ACL, PCL, or collateral ligament injuries, especially after sports trauma, twisting injuries, or sudden directional changes.
When is meniscus surgery usually discussed?
Surgery may be discussed when there is repeated true locking, a displaced tear, major trauma, or symptoms that remain limiting after an appropriate course of non-surgical care.
Is physiotherapy useful for meniscus tear care?
Registered physiotherapy may help with knee motion, strength, balance, walking mechanics, and activity progression. Exercise order and load control are important when meniscus symptoms are present.
When should I get a meniscus tear assessed?
Assessment is recommended when swelling, locking, catching, giving-way, difficulty walking, or difficulty fully straightening the knee continues after injury or keeps returning.
Page Summary: Meniscus Tear Care in KL
A meniscus tear can affect how the knee handles walking, stairs, squatting, turning, kneeling, and getting up after sitting. Symptoms may include swelling, stiffness, joint-line discomfort, clicking, catching, locking, or difficulty fully straightening the knee. The pattern depends on the tear type, tear location, knee stability, cartilage condition, and whether nearby structures such as the ACL, PCL, collateral ligaments, tendons, or surrounding muscles are also involved.
The meniscus does not work alone. Hip control, ankle mobility, foot position, walking mechanics, kneecap tracking, and lower-limb strength may all influence how much load reaches the knee. That is why assessment should look beyond the MRI label and review how the knee functions during real daily movement.
Non-surgical meniscus care may include registered physiotherapy, chiropractic joint mobilization, soft tissue methods, guided rehabilitation, activity modification, walking review, and exercise progression when appropriate. Surgery may still be discussed in selected cases, especially when true locking, a displaced tear, major trauma, or persistent mechanical symptoms are present.
For readers in Kuala Lumpur, a structured meniscus care plan should be based on the tear pattern, symptoms, imaging findings when available, swelling, stability, walking tolerance, and daily activity needs. The goal is to guide knee movement, load control, and function through assessment-led Meniscus Tear Care in KL | Non-Surgical Knee Guide.