


Occiput & Atlas (C0–C1): Dos and Don’ts in Chiropractic
The occiput and atlas (C0–C1) form the gateway between your brain and body, connecting the base of the skull to the top of the spine. This delicate joint influences posture, balance, blood flow, and nerve communication. Even subtle misalignments or tension here can trigger neck stiffness, headaches, jaw tension, dizziness, and other movement-related issues.
At Chiropractic Specialty Center® in Kuala Lumpur, we focus on gentle, non-rotatory methods for C0–C1 care — avoiding high-force or risky maneuvers that may compromise the vertebral arteries, brainstem, or surrounding ligaments.
Takeaway: Safe, Integrated Care for C0–C1 (Occiput & Atlas) Dysfunction
C0–C1 — the junction between the skull (occiput) and the first neck bone (atlas) — plays a vital role in posture, balance, nerve function, and jaw mechanics. At Chiropractic Specialty Center® in Kuala Lumpur, we manage occiput–atlas dysfunction with a detailed, step-by-step approach:
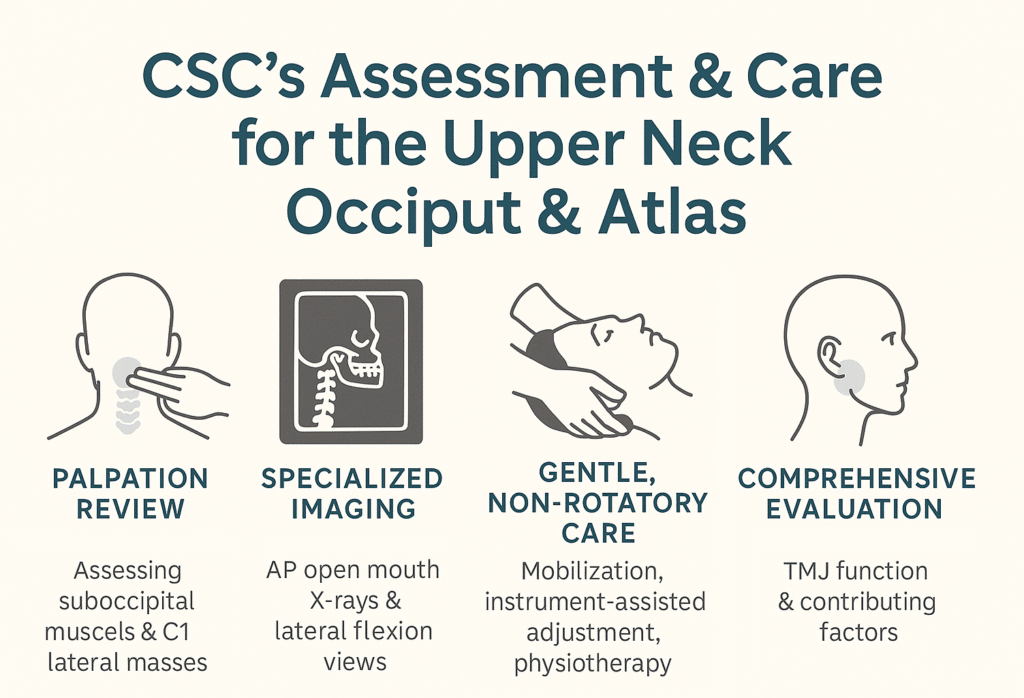
- Comprehensive Assessment – We evaluate suboccipital muscles, C1 lateral masses, and related joints, and may order specialized X-rays to detect misalignment, instability, or rotational patterns involving the occiput, atlas, and C2.
- Gentle, Non-Rotatory Correction in KL – CSC’s care for the occiput and C1 segments in Kuala Lumpur care avoids twisting or high-force traction. Instead, we use precise mobilization, instrument-assisted chiropractic adjustments, and targeted physiotherapy such as ultrasound, high-intensity laser therapy (HILT), and soft tissue release.
- Addressing the TMJ–Upper Neck Link – Because jaw function and upper neck mechanics are interconnected, we include TMJ evaluation and, when needed, jaw-focused muscle and alignment care to improve long-term stability.
This integrated, non-invasive model ensures C0–C1 correction is performed safely, addressing not just the joint itself but the surrounding muscles, nerves, and contributing factors for better function and comfort.
Understanding the Occiput & Atlas (C0–C1)
The C0–C1 segment — also known as the atlanto-occipital joint — supports head movement and protects critical structures, including the brainstem, upper spinal cord, and vertebral arteries. You can learn more about cervical spine anatomy from Cleveland Clinic
Key structures protected by the atlanto-occipital joint include:
- Brainstem & upper spinal cord
- Vertebral arteries supplying the brain
- Cranial nerves affecting balance, vision, swallowing, and jaw function
This upper neck joint allows a “nodding” motion but is not designed for aggressive twisting or yanking. Excessive force can strain ligaments, disrupt blood flow, or irritate delicate nerves.
Prevalence & Rising Neck Problems at the C0–C1 Junction
C0–C1 (occiput–atlas) instability or related dysfunction is relatively rare but clinically significant, particularly with the rising prevalence of adolescent neck disorders linked to smartphone use. Congenital variations, such as atlanto-occipital assimilation, occur in approximately 0.1–0.75% of the population (Tubbs et al., 2011; Khan et al., 2025).
Problems at the very top of your neck aren’t common, but they matter — and they’re becoming more frequent. Kids and teens who spend hours looking down at their phones are seeing more neck problems. About one in every hundred people is also born with a small structural change here that can make this area more vulnerable (Tubbs et al., 2011; Khan et al., 2025).
Neck Pain Trends Among Youth & Smartphone Use
Between 1990 and 2019, global neck pain cases among adolescents and young adults increased from 11.6 million to 12.9 million, with the highest prevalence in the 20–24 age group at approximately 109,000 per 100,000 population (Sung et al., 2023). Prolonged forward-head posture from mobile device use is a major contributor, disproportionately affecting females (Al-Khayer et al., 2024; Choudhury et al., 2025).
Neck pain in young people is climbing. In 1990, there were about 11.6 million cases worldwide — now it’s nearly 13 million. The worst-affected group? Young adults aged 20–24. Spending hours looking down at phones is a big reason, and girls tend to be affected more (Sung et al., 2023; Al-Khayer et al., 2024; Choudhury et al., 2025).
Global Burden of Neck Pain (Including C0–C1 Stress Impact)
In 2020, neck pain affected an estimated 203 million people worldwide, with projections suggesting this will increase to 269 million by 2050 — a 32.5% rise (Wu et al., 2023). Women show consistently higher prevalence rates across all age groups (Wu et al., 2023).
Right now, over 200 million people around the world have neck pain — and by 2050, that number could be almost 270 million. Women are more likely to be affected than men (Wu et al., 2023).
References for the Statistics
- Tubbs RS, et al. The anatomy of the craniovertebral junction. Child’s Nervous System. 2011;27(5):623-631.
- Khan M, et al. Anatomical study and clinical significance of occipital condyle morphology. Anatomy & Cell Biology. 2025;58(2):102-110.
- Sung YK, et al. Temporal trends in neck pain prevalence among adolescents and young adults aged 10–24 years. Archives of Medical Science. 2023;19(6):1447-1456.
- Al-Khayer A, et al. Musculoskeletal neck pain in children and adolescents: risk factors and complications. Surgical Neurology International. 2024;15:137.
- Choudhury S, et al. Association between smartphone addiction and musculoskeletal pain in children and adolescents. Frontiers in Pain Research. 2025;6:1489293.
- Wu A, et al. Global, regional, and national burden of neck pain, 1990–2020, and projections to 2050. The Lancet Rheumatology. 2023;5(6):e373-e383.
How C0–C1 Impacts the Rest of Your Neck
The joint between your skull and the top neck bone — called the occiput and atlas — isn’t just about head movement. It’s the starting point for every motion and nerve signal that travels down your neck. If C0–C1 is off balance, it can shift how the rest of your neck works:
- C1–C2 controls most of your head-turning. If it’s overworked, it can strain delicate arteries.
- C2–C3 connects upper neck movement to the middle neck and can spark headaches if it’s tight.
- C3–C4 helps with bending your neck and keeping your shoulders steady.
- C4–C5 supports shoulder lifts and even helps your breathing muscles work well.
- C5–C6 keeps your arms and wrists strong and is often stressed by poor posture.
- C6–C7 helps you grip, write, and use your hands with control.
- C7–T1 links your neck to your upper back, helping your arms move in sync.
When one part of the neck isn’t working right — especially at the top — the rest of the spine adapts, which can lead to tension, imbalance, or nerve irritation.
C0–C1 Dysfunction and Nerve Involvement
The C0–C1 joint lies near critical neurological structures, meaning even mild dysfunction can influence nerve signaling. The C1, C2, and C3 spinal nerves emerge just below the skull and help supply sensation to the back of the head, neck, and portions of the jaw. Additionally, this junction sits in close proximity to several cranial nerves, which can be affected by mechanical strain, altered blood flow, or muscle tension.
Key cranial nerves near C0–C1 include:
- CN V (Trigeminal Nerve): May be influenced through dural tension, potentially contributing to jaw or facial discomfort.
- CN VII (Facial Nerve) & CN VIII (Vestibulocochlear Nerve): Their shared passage through the internal acoustic meatus means vascular or muscular changes in the region can sometimes produce ear fullness, tinnitus, or mild balance changes.
- CN XI (Accessory Nerve): Supplies the sternocleidomastoid and trapezius muscles, both of which can be affected by atlas misalignment.
- CN XII (Hypoglossal Nerve): Close to the occipital condyles and may be influenced during excessive C0–C1 rotation or flexion.
When C0–C1 mechanics are compromised, surrounding soft tissue tension or joint malpositioning may irritate these nerves, leading to symptoms such as occipital neuralgia, dizziness, jaw tension, visual changes, and neck stiffness. Clinical imaging and precise palpation are essential to identify whether nerve involvement is structural, vascular, or muscular in origin.
References for C0-C1 Nerve Involvement
- Bogduk N. “The anatomy of occipital neuralgia.” Clin Exp Neurol. 1980;17:167–184.
- Tubbs RS, et al. “The anatomy of the craniovertebral junction.” Childs Nerv Syst. 2011;27(5):623–631.
- Piagkou M, et al. “Anatomical study of the accessory nerve: clinical implications in head and neck surgery.” Clin Anat. 2011;24(2):202–212.
Atlanto–Occipital (C0–C1) vs. Atlanto–Axial (C1–C2) Joint Function
The upper cervical spine contains two unique joints with distinct yet interdependent roles:
| Joint | Primary Motion | Approx. Motion Range | Key Functions | Common Stress Points |
|---|---|---|---|---|
| C0–C1(Atlanto–Occipital) | Flexion & extension (“nodding yes”) | ~25° flexion, ~30° extension | Allows vertical head nodding, stabilizes skull, protects brainstem | Ligament strain, vascular compression, dural tension |
| C1–C2(Atlanto–Axial) | Rotation (“shaking no”) | ~35–45° rotation to each side | Major contributor to neck rotation, maintains horizontal gaze | Facet capsule strain, transverse ligament stress |
Although C0–C1 specializes in nodding and C1–C2 in rotation, both must function in harmony. For example, excessive C1–C2 rotation without proper C0–C1 flexion control can shift the load to surrounding muscles, affecting posture and potentially irritating vertebral artery pathways.
Understanding the difference helps guide gentle, non-rotatory correction strategies at CSC, where C0–C1 care is approached with precision to protect neural and vascular integrity while improving biomechanics.
References for C0-C1 vs. C1-C2
- Dvorak J, et al. “In vivo flexion/extension of the normal cervical spine.” J Orthop Res. 1991;9(6):828–834.
- White AA, Panjabi MM. Clinical Biomechanics of the Spine. 2nd ed. Lippincott Williams & Wilkins; 1990.
- Oxland TR, Panjabi MM. “The onset and progression of spinal injury: a biomechanical perspective.” Spine. 1992;17(6 Suppl):S629–S635.
Root Causes of C0–C1 Dysfunction
Neck problems at the base of the skull or the occiput–atlas level can arise from:
- Poor posture – forward head carriage from desk or device use (Tech or Text Neck)
- Whiplash injuries – sudden acceleration/deceleration forces
- Jaw imbalance (TMJ dysfunction) – altering upper cervical mechanics
- Repetitive strain – prolonged driving, phone cradling, or side sleeping
- Disc stress in the upper neck – changing joint load patterns
- Muscle imbalance – tight suboccipital or jaw muscles restricting movement
Symptoms & Possible Effects
When C0–C1 is stressed or misaligned, patients may notice:
- Headaches or migraines
- Occipital neuralgia (sharp pain behind the head)
- Dizziness or balance changes
- Jaw tension & TMJ discomfort
- Visual disturbances or ear fullness
- Neck stiffness or movement restriction
TMJ–Upper Neck Complex Dysfunction
The jaw (TMJ) and upper neck (C0–C1) work in harmony. Dysfunction in one often disrupts the other, leading to a combined pattern of symptoms such as headaches, occipital neuralgia, dizziness, imbalance, and tinnitus.
Occiput and Altas disorder of a C0-C1 dysfunction connection exists because the muscles and nerves controlling the jaw and upper neck share overlapping pathways. When the atlas is misaligned or restricted, it can alter jaw mechanics, and when the TMJ is dysfunctional, it can change how the atlas and occiput move. Over time, this cycle can strain the brainstem and contribute to persistent discomfort and postural changes.
Atlanto–Occipital Junction & Brainstem Relevance
The atlanto–occipital junction sits directly beside the brainstem — a key control center for balance, coordination, and basic life functions. Rotational malpositioning at this level can:
- Disturb nerve signal transmission
- Affect blood flow through vertebral arteries
- Trigger neurological symptoms such as dizziness, visual changes, or tinnitus
Given the high stakes, our care for this region is always low-force, precisely guided, and non-rotatory.
Proper Assessment for C0–C1 Disorders
Before beginning care, a detailed evaluation is essential. At CSC, assessment includes:
- Palpating suboccipital muscles for tension and tenderness
- Checking the lateral masses of C1 for restrictions or misalignment
- Ordering specialized imaging when necessary:
- AP Open Mouth X-ray – to view C1, C2, and the dens
- AP Open Mouth with Right & Left Lateral Flexion – to detect lateral listhesis or instability in the occiput, C1, C2 complex
- Evaluating C2 rotation patterns, as C2 (Axsis) often rotates opposite to occiput malpositioning when C1 (Atlas) is involved
This approach ensures that any care plan is tailored to the exact biomechanical and neurological needs of the patient.
Risks of Forceful & Rotatory Methods
Some techniques marketed for upper cervical care — such as the “Occipital Lift” or “Magic Hug”— involve side-bending and upward thrusts while seated. While advertised as gentle, these can overstretch vertebral arteries, strain ligaments, and place excessive force on the brainstem region. Case reports have linked such methods to vertebral artery dissection and, in rare cases, stroke.
Beyond these rotational risks, certain aggressive neck traction methods using a towel (towel jerks) have gained popularity online — yet they raise their own set of safety concerns.
Aggressive Neck Traction Methods: Ring Dinger®, Y-Strap & Towel Jerks
Over recent years, social media has popularized neck traction maneuvers such as the Ring Dinger®, Y-Strap, and towel jerks. These methods create a sudden, high-force pull along the spine, often producing a loud popping sound.
While dramatic in videos, these are not recognized chiropractic techniques because they:
- Are not taught in accredited Doctor of Chiropractic (D.C.) programs.
- Are not part of national licensure examination standards (e.g., NBCE).
- Lack peer-reviewed evidence supporting their safety or clinical benefit.
Safety concerns include:
- Excessive traction on the cervical spine and spinal cord
- Possible overstretching of vertebral arteries and ligaments
- Risk of exacerbating undiagnosed disc or instability issues
- Documented cases linking such forceful pulls to vertebral artery dissection and, in rare instances, stroke
At CSC, we do not use these methods. Instead, we focus on gentle, non-rotatory C0–C1 care that respects anatomical limits and uses targeted mobilization supported by physiotherapy.
Gentle, Non-Rotatory C0–C1 Care at CSC
Our approach avoids twisting, yanking, or high-velocity rotation. Instead, we combine:
- Modified SNAGs & dorsal glide mobilization – precise, low-force correction of joint motion
- Instrument-assisted atlas adjustment – gentle impulse without manual rotation
- Physiotherapy modalities – ultrasound, high-intensity laser therapy (HILT), and manual muscle release for surrounding soft tissues
- Targeted rehabilitation – chin tucks, deep neck flexor training, posture retraining
- TMJ release therapy – when jaw imbalance contributes to upper cervical strain
Exercises & Self-Care (With Professional Approval)
- Occiput Micro-Nods – gentle “yes” movements while lying down (5–7 reps)
- Suboccipital Towel Release – rest your head over a rolled towel for 2–3 minutes
- Jaw-Supported Lateral Glides – slow, controlled side tilts without rotation
Always stop and seek professional care if you feel dizziness, sharp discomfort, or neurological symptoms.
Summary Table – Safe vs. Risky Options
| Avoid | Use Instead |
| Occipital Lift (“Magic Hug”) | Gentle C0–C1 glides, non-rotatory mobilization |
| Cervical rotation thrusts | Controlled mobilization with stability exercises |
| DIY neck manipulation | Clinician-guided care & safe at-home exercises |
References – Occiput & Atlas (C0–C1) Care and Safety
- Bogduk N, Mercer S. “Biomechanics of the cervical spine. I: Normal kinematics.” Clinical Biomechanics. 2000;15(9):633-648.
- Dvorak J, Panjabi MM, Novotny JE, Antinnes JA. “In vivo flexion/extension of the normal cervical spine.” Journal of Orthopaedic Research. 1991;9(6):828-834.
- Hack GD, Koritzer RT, Robinson WL, Hallgren RC, Greenman PE. “Anatomic relation between the rectus capitis posterior minor muscle and the dura mater.” Spine. 1995;20(23):2484-2486.
- Eriksson PO, Zafar H, Nordh E. “Craniofacial growth and the function of the jaw–neck motor system.” Acta Odontologica Scandinavica. 1999;57(5):275-284.
- Fernández-de-las-Peñas C, Cuadrado ML, Pareja JA. “Myofascial trigger points, neck mobility, and forward head posture in unilateral migraine.” Cephalalgia. 2006;26(9):1061-1070.
- Whedon JM, Song Y, Mackenzie TA, Lurie JD. “Risk of cervical artery dissection after chiropractic spinal manipulation in Medicare B beneficiaries aged 65 to 99 years.” BMC Geriatrics. 2022;22:917.
- Cassidy JD, Boyle E, Côté P, et al. “Risk of vertebrobasilar stroke and chiropractic care: results of a population-based case-control and case-crossover study.” Spine. 2008;33(4 Suppl):S176-S183.
- Erro R, Tinazzi M, Marinelli L, et al. “Cervical dystonia following whiplash injury: case reports and review of the literature.” Movement Disorders. 2010;25(15):2602-2606.
- Hall T, Briffa K, Hopper D. “Clinical evaluation of cervical dorsal glide mobilization for cervicogenic headache.” Manual Therapy. 2007;12(2):123-130.
- Mingels S, Dankaerts W, van Etten E, et al. “Upper cervical range of motion is restricted in patients with temporomandibular disorders.” Journal of Oral Rehabilitation. 2019;46(2):109-116.
- Fagundes CF, et al. “Strain of the vertebral artery during passive neck manipulation.” Journal of Manipulative and Physiological Therapeutics. 2014;37(9):657-664.
- Jones JG, et al. “Vertebral artery dissection following chiropractic manipulation.” Chest. 2015;147(4):e143-e147.
Conclusion
C0–C1 care should never involve guesswork or high-force maneuvers. At Chiropractic Specialty Center®, we deliver Occiput & Atlas Physiotherapy with chiropractic care in Kuala Lumpur using gentle, clinically guided methods supported by physiotherapy for safer, more effective results.
Meet the Author: Occiput & Atlas – Safe Chiropractic Care for C0–C1 Alignment
Written by Y. Zafer, who has nearly three decades of experience in gentle, non-rotatory spine care, this article on Occiput & Atlas (C0–C1): Dos and Don’ts in Chiropractic reflects an evidence-based approach to upper cervical health through integrated chiropractic and physiotherapy.
Last Updated: Occiput & Atlas (C0–C1): Dos and Don’ts in Chiropractic
This page was last updated on August 8, 2025, to ensure the latest, most accurate, and compliance-focused information on C0–C1 care.
FAQ – Occiput & Atlas (C0-C1) Chiropractic & Physiotherapy Care
The occiput is the base of your skull, and the atlas — also called C1 — is the first bone in your neck. Together, they form the C0–C1 joint, which controls head movement and protects vital structures like the brainstem, upper spinal cord, and vertebral arteries. Even a small misalignment can affect posture, balance, nerve signals, and blood flow, leading to issues such as headaches, dizziness, jaw tension, and visual changes.
The jaw joint (TMJ) and upper neck share muscles, nerves, and movement patterns. If your atlas or occiput is misaligned, it can change how the jaw moves. Likewise, TMJ tension can pull on neck muscles, altering C0–C1 motion. This “two-way link” means problems in one area often create or worsen symptoms in the other, such as headaches, tinnitus, imbalance, and chronic muscle tightness.
C0-C1 issues can produce a wide range of symptoms, including:
– Occipital neuralgia (sharp pain behind the head)
– Headaches or migraines
– Dizziness or balance problems
– Jaw discomfort or TMJ clicking
– Neck stiffness or restricted motion
– Visual disturbances or ear fullness
These symptoms often overlap, especially when TMJ involvement is present, which is why a thorough assessment is essential.
Assessment starts with a hands-on examination of suboccipital muscles and the lateral masses of C1 to detect tension, restrictions, or misalignment. If needed, specialized imaging is performed, including AP open mouth X-rays and lateral flexion views. These help identify instability, rotational malpositioning, or subtle joint shifts between the occiput, atlas, and C2. This detailed approach ensures any care is precise, safe, and tailored to your unique biomechanics.
These methods use high-force traction or rapid pulling of the spine, which can strain vertebral arteries, ligaments, and delicate brainstem structures. They are not taught in accredited chiropractic programs, are not part of licensure exams, and lack safety evidence in peer-reviewed research. At CSC, we only use gentle, non-rotatory techniques combined with physiotherapy to restore C0–C1 function safely and effectively.
Frequently Asked Question on C0-C1 Statistics
Problems at the C0–C1 joint — where your skull meets your spine — are not common, but they’re becoming more frequent. Congenital changes here occur in about 1 in 100 people, and neck pain overall affects more than 200 million people worldwide. Kids and young adults, especially females, are showing more issues from spending hours looking down at phones. By 2050, global cases of neck pain are expected to rise by more than 30 percent.
C0–C1 (occiput–atlas) disorders are relatively rare, with congenital variations like atlanto-occipital assimilation affecting 0.1–0.75% of people (Tubbs et al., 2011; Khan et al., 2025). However, global neck pain cases rose from 203 million in 2020 to a projected 269 million by 2050 (Wu et al., 2023). Adolescents and young adults, especially females, are experiencing higher rates due to prolonged forward-head posture from smartphone use (Sung et al., 2023; Al-Khayer et al., 2024; Choudhury et al., 2025).
Frequently Asked Questions on Impact to Other Cervical Segments
No part of your neck works in isolation. If C0–C1 is stiff, misaligned, or unstable, other neck joints have to compensate. This can overload the C1–C2 joint — which handles most rotation — and strain mid and lower cervical levels like C4–C5 and C5–C6. Over time, this chain reaction can affect posture, muscle balance, nerve function, and even jaw movement.
C0–C1 dysfunction alters the biomechanics of the cervical spine, forcing compensatory motion at C1–C2 (atlanto-axial joint) and increased stress at mid-cervical segments (C3–C4, C4–C5, C5–C6). This can contribute to accelerated facet joint strain, altered nerve root mechanics, and muscle imbalance patterns affecting posture and jaw function. Intersegmental dependency means that dysfunction at C0–C1 can cascade throughout the cervical spine, impacting stability and movement efficiency.