

Care Management Plan & Frequency of Therapy – First Case
Following a comprehensive consultation, a personalized NSD Therapy® program was initiated for the patient. The individual’s condition, symptoms, examination findings, and MRI impressions were entered into the Care Management Software of the RxDecom® (a spinal decompression system).
The initial phase of NSD Therapy® consisted of daily sessions (Monday-Friday) for three weeks, followed by a care schedule of three sessions per week for five weeks. The patient underwent a total of 30 therapy sessions following the NSD Therapy® protocol.

Response to NSD Therapy® – First Case
The patient showed excellent progress. By the final evaluation on April 27, 2010, there was significant improvement in overall function. The level of discomfort had reduced from a constant 9/10 to an occasional 1/10, with no recurring symptoms down the leg.
Orthopedic tests, including Valsalva’s Maneuver, Milgram’s test, and SLR, were all negative. Additionally, the Achilles reflexes were +2 bilaterally, indicating improved neurological function. To assess structural changes, a follow-up MRI scan was performed on April 29, 2010 (see Figure-2).
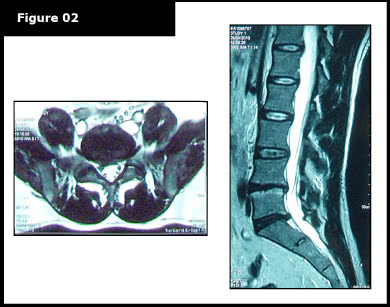
A board-certified radiologist conducted a comparative study between the new MRI and the previous MRI from November 11, 2008. The comparison showed a significant reduction of the extruded disc material, resulting in reduced compression on the spinal cord (thecal sac). Additionally, the neural foramina were intact bilaterally at L5-S1. However, at L4-L5, no significant structural changes were noted.
Second Case – Moderate to Severe Disc Extrusion
A 44-year-old male engineer of Persian descent sought care for severe lower back discomfort that extended to the left buttock, posterior thigh, and leg. The patient also reported numbness, tingling, and a burning sensation along the bottom of the left foot and big toe, as well as weakness affecting the entire lower left limb.
On a 1 to 10 scale for discomfort (1 being minimal and 10 being the most severe), the patient reported a level 10 intensity.
Upon examination:
- The patient exhibited mild left foot weakness.
- Achilles reflex was zero (0) on the left and +2 on the right.
- Due to the severity of the condition, provocative orthopedic testing was not performed to avoid exacerbating symptoms.
The patient had previously undergone two MRI scans, the first on December 29, 2009, and a second on January 23, 2010 (Figures-3 and 4).

A comparative review of the MRI scans revealed a worsening of the disc bulge observed in December 2009. The condition had progressed to a moderate disc extrusion, which significantly compressed the spinal cord (thecal sac) and S1 nerve root.

To address the condition, NSD Therapy® was recommended to promote recovery and improve function. Due to the severity of the disc condition, the patient underwent 25 therapy sessions of NSD Therapy®, administered five times per week for five weeks.
Outcome of the Second Case Through Our Proven Slipped Disc Care
The patient demonstrated continuous improvements throughout the course of therapy. By the final care session, the patient reported a complete resolution of lower back discomfort (0/10) and only an occasional mild sensation (1/10) down the leg on the visual analog scale.
The clinical evaluation performed on April 16, 2010, showed normal bilateral (+2) Achilles reflexes with no signs of foot weakness. Additionally, orthopedic tests including Straight Leg Raise (SLR), Milgram’s, and Valsalva’s Maneuver were all negative, indicating improved neurological function and stability.
A follow-up MRI scan of the lumbar spine on April 19, 2010 (Figure-5) was conducted to assess structural changes. A comparative analysis between the post-therapy MRI and the pre-therapy MRI (dated Jan. 23, 2010) revealed significant improvements, supporting the effectiveness of the NSD Therapy® approach in promoting spinal recovery.
