


C7-T1 Spine: Joint, Disc & Nerve Care in Kuala Lumpur
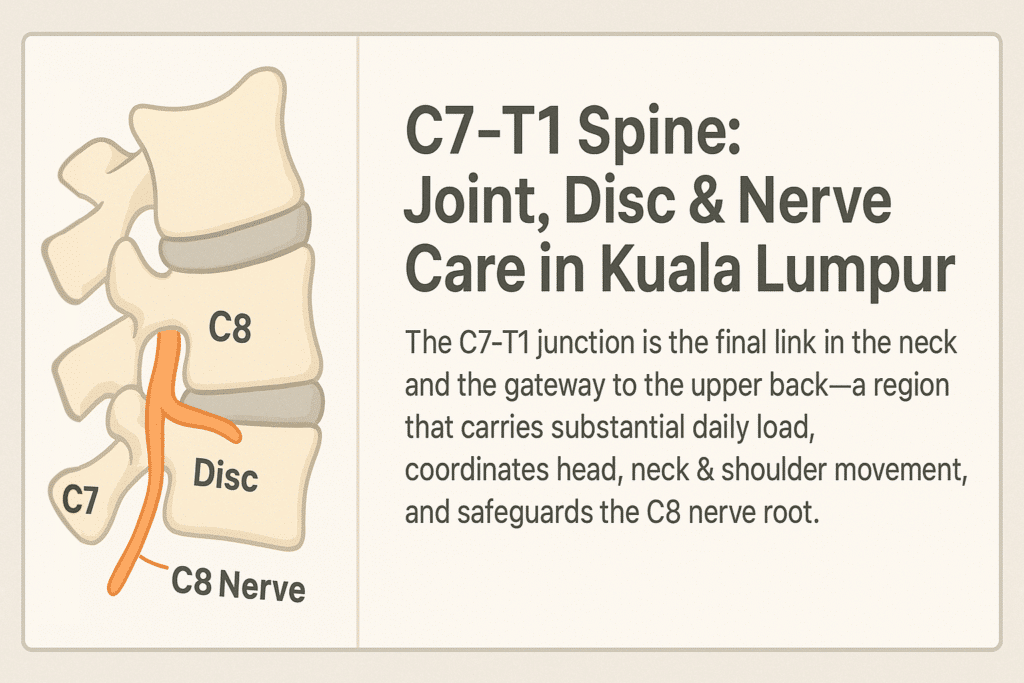
The C7-T1 junction is the final link in the neck and the gateway to the upper back — a region that carries substantial daily load, coordinates head, neck & shoulder movement, and safeguards the C8 nerve root. This nerve controls fine grip strength, finger coordination, and sensation in parts of the forearm, making C7-T1 essential for both precision and stability in upper limb function.
Changes here, whether from posture strain, repetitive stress, or structural shifts, can influence every segment above and alter how the shoulders and arms perform. In the sections ahead, you’ll learn what makes C7-T1 unique, the conditions that often develop here, how it can affect other neck levels, and the safest evidence-based approaches to restore healthy motion and nerve protection.
At Chiropractic Specialty Center® in Kuala Lumpur, our chiropractors and physiotherapists have decades of experience in integrative, non-rotatory care tailored to each patient’s age, condition, and spinal structure. If you’d like personalised input beyond what’s covered here, call our main centre at Call Us: +603 2093 1000 or SMS / WhatsApp: +60 17 269 1873 us for guidance.
Takeaway: Key Points on C7-T1 Care
- Vital Transition Zone – C7-T1 connects the mobile neck to the stable upper back, protecting the C8 nerve that controls grip strength, finger motion & part of forearm sensation.
- Common Problems – Disc bulges, herniations, arthritis, bone spurs, facet irritation, cervical ribs, and thoracic outlet compression can all occur here.
- Wider Impact – C7-T1 issues may influence other neck segments from C0–C1 down to C6–C7, leading to posture strain, radiating arm symptoms, and reduced shoulder stability.
- Risk Awareness – Avoid unsafe traction techniques like towel jerks, Y-strap pulls & “ring dinger” methods that can aggravate spinal cord & nerve roots.
- CSC’s Approach – Our Kuala Lumpur centers provide gentle, non-rotatory chiropractic care combined with targeted physiotherapy, spinal decompression & posture rehab for safer, lasting results.
How CSC’s KL Centres Can Help
At Chiropractic Specialty Center®, care for C7-T1 conditions is non-invasive, segment-specific, and posture-corrective. Our integrated approach may include:
- Gentle joint mobilization without high-velocity neck rotation.
- Spinal decompression therapy for C8 nerve pressure.
- High-Intensity Laser Therapy (HILT) for disc & nerve recovery.
- Targeted physiotherapy for posture, scapular stability & grip strength.
- Myofascial release for scalene, pectoralis minor, and upper trapezius tension.
Every plan is tailored to the patient’s age, structural findings, and activity needs — ensuring safety while restoring motion and protecting nerve health.
Understanding the C7-T1 Segment
C7–T1 is the cervicothoracic junction — a meeting point where the flexible cervical spine meets the more stable thoracic spine. Its disc cushions vertical forces, while its facet joints channel movement. The C8 nerve root exits here, travelling through the brachial plexus into the arm and hand.
Because this is a transitional zone, it’s more vulnerable to mechanical stress from repetitive movement, poor posture, or sudden loading forces like whiplash.
Neck Issues and Problems: Scope, Causes & Impact
Neck problems can arise from a range of mechanical, degenerative, and postural factors. The cervical spine houses and protects the spinal cord, supports the head’s weight, and enables multi-directional movement. Disruption in its joints, discs, or soft tissues can produce localized stiffness or radiating neurological symptoms.
Common causes include:
- Degenerative disc disease & cervical spondylosis — age-related wear reducing disc height and altering joint mechanics[Gore et al., 1986].
- Disc herniation — nucleus pulposus material pressing on spinal nerves [Radhakrishnan et al., 1994].
- Facet joint arthropathy — inflammation or degeneration of the cervical facet joints [Aprill et al., 1990].
- Postural stress — prolonged forward head posture increasing load on the cervicothoracic junction [Neumann, 2017].
- Whiplash injuries — sudden flexion-extension strains damaging ligaments and discs [Sterling et al., 2010].
Impact on daily life: Neck disorders can limit movement, cause referred arm symptoms, disrupt sleep, and affect work performance. In severe cases, they can lead to chronic disability.
References – Neck Issues & Problems
- Gore DR, et al. (1986). Roentgenographic findings of the cervical spine in asymptomatic people. Spine, 11(6), 521–524.
- Radhakrishnan K, et al. (1994). Epidemiology of cervical radiculopathy: A population-based study. Brain, 117(Pt 2), 325–335.
- Aprill C, et al. (1990). Cervical facet joint pain patterns. Spine, 15(6), 458–461.
- Neumann DA. (2017). Kinesiology of the Musculoskeletal System. Elsevier.
- Sterling M, et al. (2010). Whiplash: Clinical course and prognostic factors. J Orthop Sports Phys Ther, 40(5), 274–283.
How C7-T1 Malfunctions Affect the Entire Neck
The C7–T1 segment is the structural bridge between the neck and upper back. Any malfunction here — whether from a slipped disc (bulge or herniation), arthritic changes, bone spurs, muscle imbalance, or nerve root compression — can disrupt the entire cervical chain from the occiput–C1 down to the lower cervical spine.
Impact on upper cervical segments (Occiput–C1, C1–C2, and C2-C3):
- Increased tension in suboccipital muscles due to compensatory head positioning.
- Possible headaches, dizziness, or visual disturbances from altered biomechanics.
Impact on mid-cervical segments (C3-C4 & C4-C5):
- Secondary joint overload as they absorb more motion.
- Facet irritation and muscle guarding leading to stiffness or reduced range of motion.
Impact on lower cervical segments (C5-C6 & C6–C7):
- Acceleration of disc wear and narrowing of nerve canals.
- Radiating symptoms such as shoulder ache, upper arm weakness, or tingling in the forearm.
Nerve-related symptoms from C7-T1 dysfunction:
- Weak grip, clumsiness in fine finger movements.
- Numbness or tingling in the ring and little fingers (C8 nerve distribution).
- Loss of dexterity or forearm fatigue with simple tasks like typing or gripping objects.
Because the cervical spine functions as an interconnected system, addressing C7-T1 issues early can prevent cascading effects on multiple levels — a key principle in safe, comprehensive neck care [Fernandez-de-Las-Penas et al., 2006; Radhakrishnan et al., 1994].
Upper Cervical and C7-T1: A Two-Way Connection
The cervical spine operates as a single functional unit, meaning stress in one region often impacts others. The upper cervical spine (C0–C3) governs fine head movements and balance, while the C7-T1 junction bears heavy mechanical load as it transitions to the thoracic spine.
When C7-T1 suffers from disc narrowing, postural strain, or degeneration, compensatory changes can occur in the upper neck — leading to muscle overactivation, joint compression, and altered proprioception. Conversely, instability or stiffness in the upper cervical region can shift mechanical stress downward, accelerating wear at C7-T1.
This interconnectedness means that effective care must evaluate the entire cervical chain, not just the symptomatic level, to prevent recurring problems [Fernandez-de-Las-Penas et al., 2006].
Reference:
- Fernandez-de-Las-Penas C, et al. (2006). The influence of cervical spine dysfunction on upper quarter pain. Clin J Pain, 22(3), 230–236.
Unsafe Neck Traction Methods: Why Towel Pulls, Y-Strap & Jerking Techniques Are Risky
Certain viral or commercially marketed neck traction techniques — including towel-wrapped neck pulls, Y-Strap pulls, and abrupt “magic hug” jerks — are not recognized chiropractic methods.
These maneuvers often involve rapid, high-force distraction without segmental control. Risks include:
- Vertebral artery strain leading to vascular injury.
- Excessive ligament stretch destabilizing the spine.
- Disc injury or herniation from uncontrolled loading.
- Nerve traction injuries causing radicular symptoms.
Safe cervical care follows established, evidence-based protocols that prioritize gradual mobilization, precise segment targeting, and avoidance of high-force distraction [Haldeman et al., 2008].
Such methods should be avoided entirely — especially in individuals with undiagnosed vascular, disc, or ligamentous conditions — and replaced with clinically guided, gentle mobilization techniques.
Reference:
- Haldeman S, et al. (2008). Clinical guidelines for chiropractic care of adults. J Manipulative Physiol Ther, 31(9), 619–626.
NSD Therapy® – A Non-Invasive Option for Mid & Lower Neck Conditions
NSD Therapy® is a specialized, non-invasive program designed to address mid and lower cervical spine conditions without surgery or injections. It combines spinal decompression, targeted physiotherapy, posture correction, and gentle mobilization to reduce mechanical stress on the discs, joints, and nerves.
By focusing on controlled, segment-specific decompression and muscle rehabilitation, NSD Therapy® aims to restore joint spacing, optimize spinal alignment, and improve neck mobility. This method is particularly suitable for disc bulges, herniations, spondylosis, postural strain, and early nerve compression — all while minimizing the risks associated with high-force or rotational techniques.
Common Problems at C7-T1
- Disc protrusion or extrusion narrowing the nerve exit (foramen).
- Degenerative disc changes lowering disc height and altering mechanics.
- Facet joint irritation from postural strain or repetitive load.
- Postural rounding leading to muscle imbalance and joint compression.
Key Statistics on C7-T1 Disorders
- C7–T1 herniations make up 4–8% of cervical disc cases, but can cause disproportionate hand and grip impairment[Boden et al., 1990].
- Up to 70% of C8 nerve root compressions show measurable loss in grip strength[Sampath et al., 1999].
- Multi-level involvement with C6–C7 occurs in over 55% of chronic radiculopathy cases [Caridi et al., 2011].
- Forward head posture increases cervicothoracic disc pressure by 10–15% for every 2.5 cm of anterior head shift [Neumann, 2017]..
- C7–T1 facet joint degeneration is present in nearly 40% of adults over age 50 [Gore et al., 1986].
Spatulated & Elongated TVP at C7 – A Hidden Risk Factor
The transverse process (TVP) of C7 can vary anatomically.
- Elongated TVP: Extends further laterally than average, narrowing the space for muscles, nerves, or vessels.
- Spatulated TVP: Broad, flattened shape increasing mechanical contact with surrounding tissues.
Both variants can crowd the neurovascular structures between the neck and shoulder, predisposing individuals to thoracic outlet syndrome (TOS) symptoms — especially if combined with poor posture or repetitive strain.
Thoracic Outlet Syndrome & C7-T1 Connection
TOS occurs when nerves or blood vessels in the thoracic outlet are compressed. At C7-T1, this may be aggravated by:
- Elongated or spatulated C7 TVP narrowing the costoclavicular space.
- Cervical rib development at C7 altering the passageway for the brachial plexus and subclavian vessels.
- Disc herniation or joint degeneration at C7-T1 adding secondary nerve irritation.
Symptoms of Thoracic Outlet Syndrome or TOS can include numbness in the ring/little fingers, forearm weakness, and coldness in the hand.
Cervical Rib & Disc Disorders at C7–T1
A cervical rib is an extra rib arising from C7. It may be complete (attaching to the first rib) or incomplete (ending in soft tissue).
- In many cases, cervical ribs are silent.
- In others, they cause nerve or vessel compression, contributing to TOS.
- When combined with a C7-T1 disc herniation, both mechanical and inflammatory factors can impact nerve function — producing complex symptoms in the neck, shoulder, and hand.
Other Conditions That May Affect C7-T1
- Multi-level disc bulges involving C6–C7 & C7–T1.
- Cervicothoracic kyphosis altering load distribution.
- Facet arthropathy from chronic joint stress.
- Whiplash injuries causing ligamentous strain at the junction.
- Postural syndromes from prolonged device or desk use.
Non-Invasive Solutions for C7–T1 Conditions
At Chiropractic Specialty Center®, C7-T1 care focuses on precision and safety to avoid aggravating the spinal cord and delicate nerve roots.
Our program includes:
- Segment-specific mobilization without rotation to reduce joint stiffness
- Spinal decompression therapy to relieve disc pressure on the C8 nerve
- High-Intensity Laser Therapy (HILT) for deep tissue and nerve recovery
- Targeted physiotherapy for posture correction and upper limb strength
- Rehab exercises to restore grip, finger movement, and shoulder stability
CSC’s chiropractors and registered physiotherapists in KL work together to ensure that C7–T1 care is specific to each patient’s needs and goals.
Summary Table – C7T1 Spine
| Feature | Details |
|---|---|
| Segment | C7-T1 – Cervicothoracic junction |
| Key Functions | Transfers neck motion to upper back; protects C8 nerve |
| Common Issues | Disc herniation, degeneration, TOS from TVP/cervical rib |
| CSC Approach | Gentle chiropractic, physiotherapy, decompression therapy |
References – C7–T1 Disorders
- Boden SD, et al. (1990). Abnormal magnetic-resonance scans of the cervical spine in asymptomatic subjects. J Bone Joint Surg Am, 72(8), 1178–1184.
- Sampath P, et al. (1999). Outcome in patients with cervical radiculopathy: Prospective, multicenter study. J Neurosurg, 90(2 Suppl), 161–167.
- Caridi JM, et al. (2011). Cervical radiculopathy: A review. HSS J, 7(3), 265–272.
- Neumann DA. (2017). Kinesiology of the Musculoskeletal System. 3rd ed. Elsevier.
- Gore DR, et al. (1986). Roentgenographic findings of the cervical spine in asymptomatic people. Spine, 11(6), 521–524.
Meet the Author: C7-T1 Spinal Joint & Disc Care in Kuala Lumpur
Written by Y. Zafer, this article on C7-T1 Spine: Joint, Disc & Nerve Care in Kuala Lumpur reflects decades of experience managing cervical-thoracic conditions through chiropractic–physiotherapy integration.
Last Updated: C7-T1 Spine: Joint, Disc & Nerve Care in Kuala Lumpur
This page was last updated on August 10, 2025, to include the most up-to-date strategies for C7–T1 care.
FAQ – C7-T1 Spinal Joint, Disc & Nerve Care
Why is the C7–T1 level important?
C7–T1 links neck mobility to upper back stability and protects the C8 nerve, which controls grip strength and finger movement.
What symptoms occur with C7–T1 issues?
You may experience neck stiffness, shoulder weakness, grip problems, and tingling in the ring and little fingers.
How does CSC treat C7–T1 problems?
CSC uses gentle mobilization, physiotherapy, decompression therapy, and rehabilitation to protect nerve function and restore mobility.
Conclusion
C7–T1 issues can affect both neck function and hand dexterity. CSC’s integrated chiropractic–physiotherapy model provides safe, effective, and segment-specific care.
Summary Table – C7-T1 Spine
| Feature | Details |
| Segment | C7–T1 – cervical-thoracic transition zone |
| Key Functions | Transfers neck motion, protects C8 nerve |
| Common Issues | Disc herniation, degeneration, postural strain |
| CSC Approach | Gentle chiropractic, physiotherapy, decompression therapy |
C7-T1 Spine: Questions You Didn’t Know You Needed to Ask
Can C7–T1 issues cause hand weakness without neck pain?
Yes. The C8 nerve root exits between C7 and T1 and controls grip strength, finger movement, and part of the forearm’s sensation. If this nerve is compressed — even without neck pain — you might notice dropping objects, difficulty buttoning shirts, or weaker grip during daily tasks. This can happen when disc herniations or bone spurs at C7–T1 press directly on the nerve without irritating pain-sensitive structures in the neck.
Why is C7–T1 more vulnerable in people with poor posture?
Forward head posture and rounded shoulders put constant load on the cervicothoracic junction. Unlike the more flexible upper neck, C7–T1 is a transition zone with limited mobility. Over time, this load can flatten the disc, irritate the facet joints, and cause muscle imbalances — making this segment more prone to degeneration and nerve compression.
Can C7–T1 problems affect shoulder mobility?
Yes. The C8 nerve contributes to muscle control in the shoulder girdle. Compression at C7–T1 can weaken muscles that stabilize the shoulder blade, leading to reduced arm elevation, shoulder fatigue, or compensatory strain in the rotator cuff. Patients often mistake this for a shoulder-only problem when the root cause is in the neck.
How is C7–T1 different from other cervical spine levels?
Most cervical levels are surrounded by other mobile neck joints. C7–T1, however, sits between the flexible cervical spine and the rigid thoracic spine. This makes it a stress concentration point, especially during heavy lifting, repetitive upper limb work, or high-impact sports. Its nerve root (C8) also serves very specific hand and forearm functions, so damage here produces a distinctive symptom pattern.
Why are high-force traction and Y-strap pulls risky for C7–T1?
High-force or uncontrolled traction methods — such as the Y-strap, towel pulls, or “ring dinger” — can overstretch ligaments, irritate nerve roots, and even stress the spinal cord at the cervicothoracic junction. Because the C7–T1 area is anchored to the less flexible upper back, sudden traction forces are unevenly distributed, increasing the risk of injury. Safe care should focus on controlled, segment-specific mobilization rather than forceful jerks.