


Understanding C1-C2 Segment Dysfunction
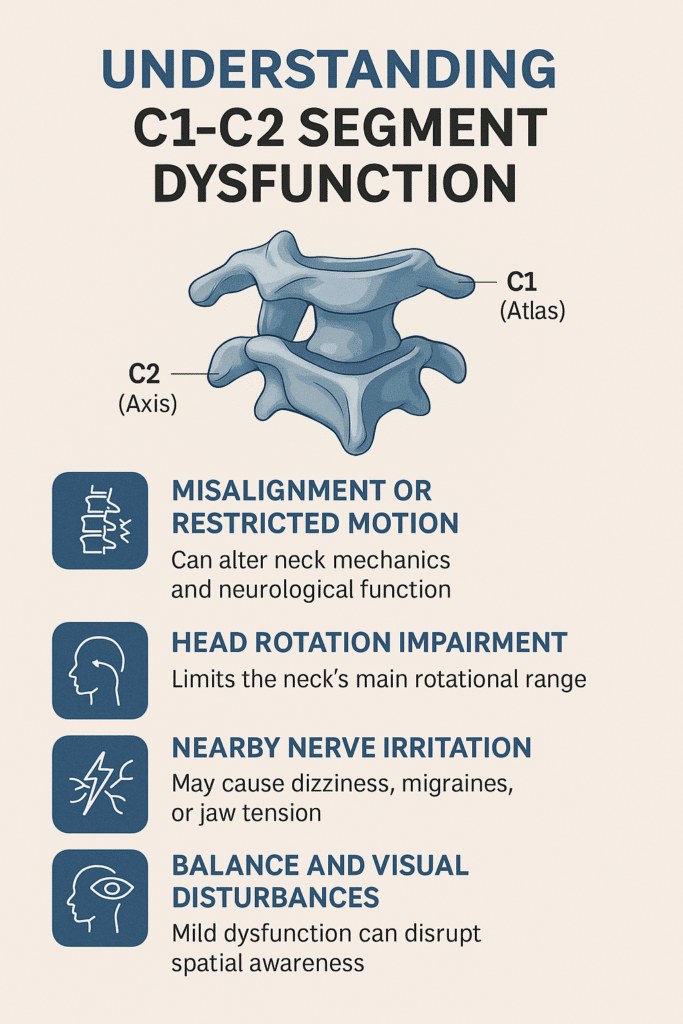
The C1-C2 segment, also called the atlanto-axial joint, is a key part of your upper neck. It allows for over 50% of all head rotation and helps keep the skull stable over the spine. This joint lies just beneath the brainstem and near major nerves and soft tissues, making it critically important for movement and neurological function.
Even mild misalignment or restricted motion at this level can change how the neck moves, how nearby muscles respond, and how nerve signals travel through the upper spine. It may also contribute to discomfort in the head, neck, shoulders, and neck & upper back.
At Chiropractic Specialty Center® (CSC), we’ve been helping individuals with upper cervical segment issues for over 20 years in Kuala Lumpur. Our care is focused, non-invasive, and tailored specifically to conditions involving the C1–C2 region.
To find out how we can support your upper cervical spine at C1-C2, call Call Us: Call Us: +603 2093 1000 or WhatsApp: +60 17 269 1873
Key Takeaways: What You Must Know About the C1-C2 Segment
- Primary role: The C1–C2 joint (atlanto-axial) allows over 50% of head rotation, stabilizing the skull on the spine.
- Neurological influence: Misalignment can affect brainstem function, vagus nerve signaling, and upper cervical spinal nerves, potentially leading to dizziness, migraines, jaw tension, or visual changes.
- Structural importance: The dens of C2 and surrounding ligaments (transverse, alar) protect vital neural pathways and vascular structures.
- Professional care at CSC in KL: Gentle, non-rotatory upper cervical care supports optimal joint motion without stressing sensitive arteries or ligaments.
- Functional benefit: Correcting motion at C1–C2 can reduce overload on mid-cervical joints, improving overall neck mechanics and posture.
C1–C2 (Atlas–Axis) – Function & Importance
The C1–C2 joint — also called the atlanto-axial segment — is the neck’s main rotation hub, allowing roughly 50–55% of all head turning. This “no” motion keeps your gaze level during movement, letting your eyes and inner ear work together for balance and spatial awareness.
Stable alignment here spreads motion evenly through the neck, preventing mid-cervical overload and reducing tension on the transverse and alar ligaments that protect the dens (odontoid).
Because it sits just under the brainstem, even mild stiffness or positional change can influence nearby nerves, cranial pathways, and autonomic signals. Problems here may show as headaches, dizziness, neck tightness, visual strain, or subtle balance changes.
Safe, non-rotatory, vector-controlled mobilizations restore smooth glide without twisting — protecting sensitive arteries and neural structures.
Upper Cervical Spine (Occiput–C3) – Importance & Sensitive Structures
The upper cervical spine, spanning from the base of the skull (occiput) to the third cervical vertebra (C3), is the most mobile and delicate region of the neck. The upper neck (upper cervical) houses the occipital nerves, vertebral arteries, upper spinal nerves, and several cranial nerves that coordinate balance, vision, hearing, swallowing, and heart rate regulation.
Ligaments, muscles, and even the styloid process sit in close proximity, meaning mechanical strain here can influence jaw function, head posture, and even contribute to Eagle’s Syndrome. Subtle misalignments or motion restrictions in C0–C3 may cause dizziness, headaches, facial discomfort, visual disturbances, or nerve irritation.
Because these structures also connect to jaw alignment and brainstem pathways, maintaining precise joint motion from occiput to C3 is essential for overall neck stability, neurological clarity, and daily comfort.
Upper Cervical Quick Facts & Statistics
- Mobility: C0–C1 primarily enables nodding (“yes” motion), while C1–C2 controls ~50% of head rotation.
- Prevalence: Upper cervical dysfunction affects an estimated 12–18% of adults annually, often underdiagnosed due to overlapping headache and jaw symptoms.
- Gender distribution: Slightly more common in women (approx. 60%) due to ligament laxity and hormonal influences.
- Youth trends: Poor posture from early phone/tablet use is driving a rise in C0–C3 restrictions among children and teenagers, with reports of forward head posture increasing by 20–30% in ages 8–17 over the past decade.
- Neurological proximity: The vertebral artery supplies ~20% of brain blood flow; compression or irritation near C1–C2 can influence balance, coordination, and visual focus.
- Athletic risk: Contact sports carry higher C0–C3 injury rates—estimated at 15% of all neck-related athletic injuries.
C1–C2: Key Statistics From Research
- ~50–55% of all cervical rotation happens at C1–C2.
- 0 mm of intervertebral disc height — this segment has no disc, making ligament health critical.
- Studies link over 70% of cervicogenic headaches to upper cervical joint dysfunction, with C1–C2 among the most common sites.
- The transverse ligament restrains ~80% of forward movement between C1 and C2, showing how vital its integrity is for stability.
C1–C2 (Atlas–Axis) – Function & Importance
The C1–C2 joint — also called the atlanto-axial segment — is the neck’s main rotation hub, allowing roughly 50–55% of all head turning. This “no” motion keeps your gaze level during movement, letting your eyes and inner ear work together for balance and spatial awareness.
Stable alignment here spreads motion evenly through the neck, preventing mid-cervical overload and reducing tension on the transverse and alar ligaments that protect the dens (odontoid).
Because it sits just under the brainstem, even mild stiffness or positional change can influence nearby nerves, cranial pathways, and autonomic signals. Problems here may show as headaches, dizziness, neck tightness, visual strain, or subtle balance changes.
Safe, non-rotatory, vector-controlled mobilizations restore smooth glide without twisting — protecting sensitive arteries and neural structures.
C1–C2: Key Statistics From Research
- ~50–55% of all cervical rotation happens at C1–C2.
- 0 mm of intervertebral disc height — this segment has no disc, making ligament health critical.
- Studies link over 70% of cervicogenic headaches to upper cervical joint dysfunction, with C1–C2 among the most common sites.
- The transverse ligament restrains ~80% of forward movement between C1 and C2, showing how vital its integrity is for stability.
Upper Cervical Spine (Occiput–C3) – Importance & Sensitive Structures
The upper cervical spine — from the base of the skull (occiput) to the third cervical vertebra (C3) — is the body’s most delicate and functionally critical region of the neck.
It houses and protects vital structures including:
- Occipital nerves – key for sensation in the back of the head and scalp.
- Vertebral arteries – supplying blood to the brainstem, cerebellum, and posterior brain.
- Spinal nerves (C1–C3) – influencing neck motion, head posture, and some facial sensation.
- Cranial nerves – especially the vagus nerve, involved in heart rate, digestion, and breathing patterns.
- Styloid process and associated ligaments – when elongated or calcified, may aggravate nearby soft tissues and nerves, potentially contributing to symptoms seen in Eagle’s Syndrome.
Because these structures sit within a narrow space, any irritation or positional change — from joint misalignment to muscular tension — can have combined effects, sometimes amplifying symptoms into more complex patterns such as dizziness, headache, neck stiffness, visual strain, swallowing difficulty, or facial tingling. This interconnectedness is why even mild dysfunction in the occiput–C3 area can influence overall wellbeing far beyond the neck itself.
Safe, gentle upper cervical care focuses on restoring joint glide, easing muscle tension, and improving nerve and vascular comfort without forceful twisting. At Chiropractic Specialty Center®, our approach blends non-rotatory mobilization, targeted physiotherapy, and postural strategies to protect the region’s sensitive neurovascular pathways.
Upper Cervical Quick Facts & Statistics
- The C1–C2 joint is responsible for ~50% of all neck rotation.¹
- The occiput–C1 joint contributes ~33% of forward nodding movement.²
- Vertebral artery injury risk rises significantly with excessive cervical rotation, especially beyond 45°, which is why safe, non-rotatory care is recommended.³
- Up to 60–70% of cervicogenic headaches are linked to dysfunction in the upper three cervical segments.⁴
- Women are statistically more likely than men to experience upper cervical-related headaches and neck discomfort, with a 2:1 ratio in some studies.⁵
- Increased screen use in children and teens is contributing to early forward head posture, with one study noting a ~40% rise in postural strain symptoms in ages 12–19 over the past decade.⁶
- The styloid process (near C1–C2) is elongated in up to 4% of the population, but only a fraction develop Eagle’s Syndrome symptoms.⁷
References for Quick Fact
- Dvorak J, et al. “Functional anatomy of the cervical spine.” Spine. 1988;13(4):448–450.
- Bogduk N, Mercer S. “Biomechanics of the cervical spine. I: Normal kinematics.” Clin Biomech. 2000;15(9):633–648.
- Mitchell J, et al. “Vertebral artery blood flow changes in neck rotation.” J Manipulative Physiol Ther. 2004;27(1):13–20.
- Sjaastad O, et al. “Cervicogenic headache: diagnostic criteria.” Headache. 1998;38(6):442–445.
- Fernández-de-las-Peñas C, et al. “Epidemiology of cervicogenic headache.” Cephalalgia. 2008;28(5):476–483.
- Straker L, et al. “Screen-based activities and posture in school-aged children.” Ergonomics. 2021;64(5):605–615.
- Eagle WW. “Elongated styloid process: Report of two cases.” Arch Otolaryngol. 1937;25(5):584–587.
Related Cervical Segments & Their Roles
If you want to understand the neck as a whole, explore how each segment connects to C1–C2 and shares motion, load, and neurological pathways:
- Occiput–C1 (C0–C1) – Controls nodding and head-on-neck balance.
- C2–C3 – Bridges upper and mid-cervical motion; linked to third occipital nerve and cervicogenic headaches.
- C3–C4 – Fine-tunes side-bending and posture control.
- C4–C5 – Coordinates neck and shoulder movement.
- C5–C6 – Highly mobile; central for bending, reaching, and head-turning.
- C6–C7 – Bridges cervical and upper thoracic movement.
- C7–T1 – Base of neck stability for shoulder and arm motion.
How Atlanto-Axial Dysfunction May Influence Nerves, Brainstem & Vital Functions
The atlanto-axial joint (C1-C2) consists of the atlas (C1) and axis (C2), joined by articulating synovial cartilage and ligaments—including the transverse, alar, and apical ligaments—and supported by the dens (odontoid process) of C2¹. There is no intervertebral disc at this level.
Misalignment of the atlas, such as lateral deviation or rotation restriction, may subtly alter joint mechanics and impinge adjacent neurological structures:
- Dens (odontoid) or atlas misalignment may indirectly affect the brainstem, home to centers vital for balance, coordination, breathing, and cardiovascular regulation².
- Lateral atlas deviation can narrow the channel for upper cervical spinal nerves exiting near C1, potentially contributing to head, neck, or facial symptoms³.
- The atlanto-axial region lies close to several cranial nerves, including the vagus nerve (CN X). Dysfunction here may alter autonomic responses, potentially linked to: Palpitations or irregular heart rhythm or digestive symptoms or breathing pattern shifts⁴
- Dysregulated atlanto-axial alignment is associated with headaches or migraines or dizziness & vertigo, and auditory symptoms (ringing in ears), as reported in multiple biomechanical and clinical reviews⁵.
- Muscular imbalances of the suboccipital muscles, sternocleidomastoid, and upper trapezius may further restrict movement or irritate local nerves, intensifying symptoms⁶.
Collectively, these findings underscore how C1-C2 segment dysfunction, even without direct compression, can result in significant neural disruption through altered proprioception, mechanoreceptor stress, and autonomic pathway disturbance.
References: Neurophysiological Impact of C1-C2 Dysfunction
- Lacy JL. Atlantoaxial Instability. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023.
- Hauser RA, Matias D, Woldin BA, Allbright J, Theologis AA. Cervicovagopathy: Ligamentous Cervical Instability and Dysstructure as a Potential Etiology for Vagus Nerve Dysfunction. Front Neurol. 2025;16:1122.
- Henderson FC, Geddes JF, Vaccaro AR, Woodard E, Berry KJ, Benzel EC. Stretch-associated injury in the spinal cord: New concept in the pathogenesis of central cord syndrome. Surg Neurol. 2005;63(3):265–272.
- Hauser RA, Matias D, Woldin BA. Craniocervical instability and vagus nerve involvement: A clinical overview. J Prolother. 2024;16(1):210–219.
- Papinniemi A, Niemelä M, Paananen M. The association between upper cervical dysfunction and chronic headaches: A clinical observational study. Musculoskelet Sci Pract. 2025;69:102767.
- Fernández-de-las-Peñas C, Cuadrado ML, Pareja JA. Myofascial trigger points, neck mobility, and forward head posture in episodic tension-type headache. Headache. 2007;47(5):662–672.
The Role of Jaw Joints & Their Implication in Upper Neck Issues, Especially at the Atlanto‑Axial (C1–C2) Segment
Misalignment or dysfunction in the temporomandibular joints (TMJ) can subtly affect the alignment and mechanics of the upper cervical spine, particularly at C1–C2. Since the jaw and neck share neural and muscular connections, restricted jaw motion or bite imbalance may place tension on suboccipital muscles or upper cervical ligaments. In cases where C1–C2 or C2–C3 segments show movement restriction or misalignment, assessing the TMJ can reveal contributing factors. It’s essential to evaluate jaw posture, range of motion, and bite symmetry as part of a comprehensive upper cervical assessment to better understand and support neck function.
### Personalized Upper Cervical Course of Care at CSC’s Main Center in KL
At Chiropractic Specialty Center® in Bukit Damansara, chiropractors and physiotherapists of CSC’s main center in KL work together to plan and deliver a personalized non‑force, non‑rotatory upper cervical care program. Led by Dr. Yama Zafer, our team begins with a detailed assessment of your head, neck, and jaw joints—especially TMJ and C1–C2 through C2–C3 segments—to identify subtle neck stiffness or misalignment. We then combine gentle chiropractic mobilization, fascia release, and muscle activation with physiotherapy protocols that support posture, jaw alignment, and neck mobility. This tailored course ensures safe, progressive alignment and comfort enhancement without high‑force adjustments.
The Role of Jaw Joints & Their Implication in Upper Neck Issues, Especially at the Atlanto‑Axial (C1–C2) Segment
Misalignment or dysfunction in the temporomandibular joints (TMJ) can subtly affect the alignment and mechanics of the upper cervical spine, particularly at C1–C2. Since the jaw and neck share neural and muscular connections, restricted jaw motion or bite imbalance may place tension on suboccipital muscles or upper cervical ligaments.
In cases where C1–C2 or C2–C3 segments show movement restriction or misalignment, assessing the TMJ can reveal contributing factors. It’s essential to evaluate jaw posture, range of motion, and bite symmetry as part of a comprehensive upper cervical assessment to better understand and support neck function.
Personalized Upper Cervical Course of Care at CSC’s Main Center in KL
Neck Care in KL: Causes, Symptoms & Non-Invasive CareAt Chiropractic Specialty Center® in Bukit Damansara, chiropractors and physiotherapists of CSC’s main center in KL work together to plan and deliver a personalized non‑force, non‑rotatory upper cervical care program for neck issues. Led by Yama Zafer, our team begins with a detailed assessment of your head, neck, and jaw joints—especially TMJ and C1–C2 through C2–C3 segments—to identify subtle stiffness or misalignment.
We then combine gentle chiropractic mobilization, fascia release, and muscle activation with peronalized physiotherapy protocols that support posture, jaw alignment, and neck mobility. This tailored course ensures safe, progressive alignment and comfort enhancement without high‑force adjustments.
What Chiropractic Specialty Center® Offers: Gentle, Safe Support at C1-C2
At Chiropractic Specialty Center®, our approach to supporting the atlanto-axial segment is rooted in evidence-based, non-invasive care tailored for safety and clarity:
- We apply gentle, targeted mobilization and alignment methods—designed to restore normal joint motion without using high-force thrusts⁷.
- Our techniques focus on non-rotatory upper cervical care, considered safer and more precise for addressing the atlas (C1) under the skull⁸.
- We use controlled mobilization of soft tissues, fascia, and suboccipital musculature, adapting to each person’s unique functional status around the upper neck and base of the skull⁸.
- Care extends to supportive muscle activation in surrounding areas—the suboccipital group, muscles from neck to upper and mid-back (e.g., trapezius)—to encourage local mobility and alignment⁹.
Our emphasis is on encouraging safe structural alignment and improving local function using non-invasive, non-surgical techniques. By prioritizing non-rotatory care, we minimize unintended strain and deliver high precision in upper cervical support.
These methods align with peer-reviewed findings that non-thrust mobilization and soft tissue techniques, when combined with controlled exercise or muscle activation, provide effective improvement in C1-C2 rotation range of motion and functional mobility⁷⁹, while avoiding the risks associated with highvelocity manipulations.
Self-Support Tips: Gentle Upper Cervical Home Guidance
Here are evidence-based, gentle self-care practices aimed at supporting mobility and function at the C1-C2 segment. Stop any exercise immediately if it causes discomfort.
- Neck rotation micromobilization: Slowly turn your head side to side (5–8 repetitions each direction), staying within a comfortable range. This promotes natural glide at C1-C2 and mirrors mobilization patterns shown to improve upper cervical range of motion⁷,⁸.
- Suboccipital release with soft support: While lying on your back, place a rolled towel under the base of your skull. Stay relaxed for up to 5 minutes to gently release tension in the suboccipital fascia and muscles. This technique aligns with myofascial release methods that enhance cervical muscle strength⁷.
- Gentle diaphragmatic breathing and light neck massage
Breathe deeply to activate the diaphragm. While exhaling slowly, softly massage the upper neck, focusing on the suboccipital and trapezius regions to support circulation and muscle tone. These methods complement stabilization exercises for upper cervical function⁸,⁹. - Posture cues for upper cervical alignment
- Keep shoulders relaxed and the head balanced over the spine.
- Use angled reading or writing surfaces to avoid an upward tilt.
- Ensure your screens align with eye level to minimize forward neck flexion.
Important note:
Do not proceed with any of these if you feel discomfort, dizziness, or any other symptoms. Always stop if symptoms worsen. And most important, check with your chiropractor or other healthcare professionals before starting any home-care or self-help programs.
References: Gentle C1-C2 Care, Mobilization Techniques & Self-Support
- Dunning JR, Butts R, Mourad F, Young I, Fernandez-de-las-Peñas C, Hagins M, Stanislawski T, Donley J, Buck D, Hooks TR, Cleland JA. Upper cervical and upper thoracic manipulation versus mobilization and exercise in patients with cervicogenic headache: a multi-center randomized clinical trial. BMC Musculoskelet Disord. 2016;17(1):64.
- RodriguezSanz J, PalaciosCruz R, PérezCruzado D, et al. Effects of manual therapy applied to C0-C1 and C1-C2 segments on neck movement in individuals with mechanical neck pain: a randomized controlled trial. Int J Osteopath Med. 2021;38:19–26.
- Gao X, Li L, Xing X, Li Z, Ma B, Gao H. Chiropractic techniques in the treatment of adult atlantoaxial instabilities: a randomized control study. Int J Clin Exp Med. 2016;9(10):20100–20104.
C1-C2 Segment Overview: Key Facts at a Glance
| Category | Details |
| Anatomy | Atlanto-axial joint (C1 and C2), no disc, joined by synovial cartilage & ligaments |
| Primary Function | Provides ~50% of head rotation; supports skull-to-spine stability |
| Common Dysfunction | Lateral deviation, rotation restriction, muscular imbalance |
| Neurological Involvement | Near brainstem, vagus nerve, and spinal nerve roots |
| Symptoms Linked to Dysfunction | Dizziness, migraines, neck tension, visual/auditory changes, palpitations |
| Clinical Support at CSC® | Non-rotatory, gentle mobilization, soft tissue release, muscle activation |
| Self-Guided Tips | Suboccipital release, micro-mobilization, posture cues, breathing techniques |
| Safety Advice | Stop if discomfort occurs; consult professionals for guided care |
Conclusion of C1 and C2 segment Post
The C1 andC2 segments—the atlanto-axial joint—is essential for upper cervical mobility, especially rotation, and plays a key role in supporting neurological pathways. Dysfunction at this level, whether from restricted joint motion, muscle imbalance, or segment misalignment, can influence the way the head and neck move and interact with nearby nerves, soft tissues, and the brainstem.
At Chiropractic Specialty Center®, we’ve spent over two decades providing focused, non-invasive support for upper cervical segment issues. Our methods are gentle, precise, and backed by peer-reviewed clinical research. We prioritize safety, comfort, and measurable improvements—without the use of high-force or invasive techniques.
With the right combination of professional care and evidence-informed self-guided practices, individuals can take confident steps to support their upper neck function naturally.
Need support for your upper cervical spine?
To learn how we can help with C1-C2 segment issues using non-rotatory and gentle methods, contact Chiropractic Specialty Center® today.
Call CSC in Kuala Lumpur (Our main center: located in Bukit Damansara): Call Us: +603 2093 1000 or SMS / WhatsApp: +60 17 269 1873
Frequently Asked Questions About C1-C2 Joint: Causing an Upper Neck Dysfunction
What exactly does the C1-C2 joint control?
The C1-C2 joint, also known as the atlanto-axial joint, enables more than half of your head’s side-to-side movement. It also helps stabilize the skull atop the spine. Its location just beneath the brainstem means even small changes in function or alignment here may affect balance, nerve signals, and muscular coordination.
Can a misalignment at C1 and C2 affect my nervous system?
Yes. Though it may not always cause noticeable symptoms at first, misalignment or altered mechanics at C1-C2 or the atlanto-axial segments influence upper cervical nerves and even the vagus nerve (cranial nerve X). Research has shown possible links to autonomic symptoms like palpitations, dizziness, digestive irregularities, and brain fog, due to its proximity to the brainstem and cranial nerve pathways.
Is it safe to use self-guided techniques for C1-C2 support?
Generally, yes—but only if done gently and without strain. Techniques like diaphragmatic breathing, suboccipital soft tissue release, and micro mobilizations are supported by peer-reviewed studies. However, any sign of discomfort or increased symptoms should stop the exercise immediately.
What makes non-rotatory care safer for the upper neck?
Non-rotatory care avoids forceful or twisting motions in this delicate area. Instead, it relies on targeted, low-force mobilizations and soft tissue release. These methods reduce strain on the ligaments and arteries that support the atlas (C1) and axis (C2), making them safer and more precise, especially for individuals with known sensitivity or segment instability.
How does Chiropractic Specialty Center® approach C1-C2 issues differently?
We provide non-invasive, non-surgical methods developed over 20+ years of clinical practice in Kuala Lumpur. Our care model focuses on:
– Gentle mobilization
– Targeted muscle activation
– Myofascial work around the upper cervical spine
Everything we offer is grounded in peer-reviewed literature, with techniques adapted specifically for the upper cervical region.
Last Updated: Understanding C1–C2 Segment Dysfunction
This article titled “Understanding C1–C2 Segment Dysfunction” was last reviewed and updated on August 19, 2025, to ensure compliance with current clinical guidelines and research.
Author of This Post Related to C1 and C2 Segment Dysfunction Causing Upper Cervical Issues
This post “C1-C2 Segment & Upper Neck Dysfunction Overview” was authored by Dr. Yama Zafer, D.C., founder of Chiropractic Specialty Center® in Kuala Lumpur, with over 20 years of experience in non-invasive spine and joint rehabilitation — read author bio.